WELCOME to those in my Microbiology classes by DRHicks
If you are in a HICKS MICROBIOLOGY class, please read the information under the menus on the right-hand side of this page and all of the information below...PLEASE DO THIS ASAP... THANKS DRH *STUDENTS: My philosophy of education is that you are capable of anything. No matter where you start. I am here to make sure you realize that potential. So here are a few self-learned secrets to an "A" & success in Microbiology: (1)attend EVERY class & PRINT/RENT/OBTAIN OUR Lab Manual 5th Ed before the end of week 2 (2)keep up, watch the videos/notes & read the assignments lightly BEFORE the lectures to prepare for a short PRETEST AT 7 PM or before class on CANVAS (3)communicate any problems EARLY, (4) interact with your instructor and classmates and stay involved/set up a study group in a class Discord(5)earn ALL the Class BONUS POINTS & earn the LRB 100 points of video notes in for every video on our UTube list; THERE WILL BE 100+, (6) earn the Sunday Zoom Help Sessions points by attending at 3PM for Questions & HELP BONUS POINTS FOR 2 QUESTIONS) (7) Start a STUDY GROUP OF 4 & PRACTICE MY OLD EXAMS NOW/WEEKLY (8)PRINT THE PPs & ASK QUESTIONS IMMEDIATELY - DON'T WAIT! - Remember, no problem is too big that we cannot solve together IF YOU COMMUNICATE in time and with sincerity.
If you keep trying and improving, you will succeed! Do not worry or panic, one step at a time + COMMUNICATION!
+Be a Volunteer! NOTE: The CALENDAR is only a guide, as we may move assignments by 1-2 classes depending on the class's speed. When we finish a section, we WILL have the evaluation SOON -- all evaluations will have an AGENDA notice at least 1 week before
DRHicks
hicksmicro@gmail.com
This is my personal email address and is to be used for student contact for daily immediate class questions
400 pointsExam 1 Laboratory Practical 1 over:VOCAB! All lectures, SCIENCE vs Pseudoscience, all PPs, & videos Textbook Chapters: 1, 2, 3, 4,& 9 plus all Laboratory in class work
400 pointsExam 2 Laboratory Practical 2 (MIDTERM) over: VOCAB!All Lectures, All Videos, Chapters: 5, 6, 7, & 8, All Lab + the ENTIRE M-20 LABORATORY GUIDE
300 POINTS LAB RECORD BOOK FROM: LAB DATA, 100 VIDEO NOTES & SIGNATURES
300 POINTS Formal typed Unknown Report
100 POINTS CLASS & ZOOM ATTENDANCE
200 POINTS Class, lab, and CANVAS participation
+250 Volunteer POINTS BONUS POINTS
2000 TOTAL CLASS POINTS:
A=1800; B=1600, C=1400; D=1200 F=<1199
EARNING CLASS BONUS POINTS (10%)
90-100% attendance = 20 pts
Before class computer setup person, Class attendance secretary, Class Discord Coordinator
Influenza/CoViD Vaccines 5pts/each
BEFORE & AFTER CLASS room checkers, sink cleaners, scope checkers, board cleaners & media storage checkers
Being a Volunteer involves deciding what you want to do to help out in class for the class Bonus Points - to prove your effort, your LRB is signed on the inside cover at midterm & in your last class: (a) class projector/computer set up before and after class shutdown (2 people); (b) West sink cleaner after class (2); (c) East sink cleaner after class (2); (d) before class scope cleaners (3); (e) after class scope CHECKERS (3); (f) attendancesecretary roll assignment keeper (2); (g) after class classroom checkers chairs/tables/board & lock-up (4); (h) Discard CHECKERS (2)
Thank you! DRH
M20 Website Fall 2026 ANNOUNCEMENTS:
Intro to class Zoom Sunday 3 PM
Spring 2026- AGENDA Week 1
*Buy your supplies early:(1) a Medium point (not any other color/not a FINE POINT!) BLACK "click to close type" Sharpie marker, (2) a fireplace butane lighter , (3) a small bottle of hand sanitizer, (4) a small set of colored pencils, (5) a Dark BLACK writing pen, (6) a can of "Bon Ami or Bartender's Friend" scouring powder (No substitutes), (7) buy SEVERAL #2 pencils with GOOD ERASERS, (8) select a "loaner" or buy a long sleeve to the knees WHITE cotton or cotton/mix Lab Coat ($10 on Amazon) & (9. very IMPORTANT!)*****BUY a small personal battery fan, OPTIONAL: A BOX OF NITRILE GLOVES THAT FIT YOU (NOT STERILE) and a small bottle of cheap fingernail polish remover
YOU DO NOT HAVE TO BUY: A TEXTBOOK or a FACESHIELD
*LOOK OVER THIS WEBSITE - click on EXAM 1 ALL (RIGHT MENU BUTTON)
* From Exam 1 select notes and download, print, and READ the 1st PowerPoint "INTRO TO Science."What is SCIENCE? vs Pseudoscience? BE ABLE TO DISCUSS THE DIFFERENCES THAT DISTINGUISH SCIENCE FROM PSEUDO-SCIENCE!
* For the TEXTBOOK (See Microdropbox Test & Ancillary Materials) read and review Chapters 1 and 2, "Why Study Microbiology & Review of Simple Chemistry" on your own. Always know the Chapter Vocabulary like: atoms, compounds & Periodic Chart.
* I will send you the Zoom link for Sunday's 3pm session on Friday, or look at the Canvas Calendar. ATTENDANCE or viewing the recording IS REQUIRED!
*CLASS Attendance is mandatory. If you miss 2 classes or skip the first class, you will be dropped - late is OK. If "something important comes up," TEXT ME before CLASS. You will receive SIGNIFICANT BONUS POINTS IF YOU HAVE 90% ATTENDANCE!
1) GO TO hicksmicro.blogspot.com AND DOWLOAD THE FIRST PowerPoint "SCIENCE" - READ IT FOR THE THURS CLASS ALSO DO THE SAFETY PAGE & THIS INDEX PAGE FOR PRETEST TEST 1
3) The PLAYLIST VIDEOS - ALL videos in the Lab Guide Playlist - Online MicroUtube Videos are at hicksmicro on YouTube PLAYLIST 1 Exam LP1! handwrite these in your LRB by date and during that ASSIGNMENT DISCUSSION. NO TYPED
YOU MUST READ & RECORD on YOUR daily class AGENDA in your LRB
Find OUT WHERE TO FIND THE CLASS VIDEOS & MICRODROPBOX on the website. READ "How to get an "A" & How to send me an Email on the index or first page - bottom.
(CLICK HERE for CLASS VIDEOS). Take LRB notes from each video as ASSIGNED, no matter how short (however you wish; story, outline, bullet-points) for each video on a separate page, put the video title and the date you watched it, & TAKE HANDWRITTEN your notes.
Micro is not intellectually "HARD," but there is a huge amount of material moving very fast - YOU MUST KEEP AHEAD! Do NOT miss 1 day and plan to attend the out-of-class HELP/Practice Sessions.
DRHicks 213-421-5777 emergency text only hicksmicro@gmail.com class questions Look in the Microdropbox - click on the links - TEXT ETC.!
View ALL my UTUBE videos ASSIGNED under each Exam *Many of the Lectures and ALL OF THE REQUIRED CLASS VIDEOS may be seen at: (CLICK HERE for CLASS VIDEOS)
See the daily AGENDA posted on the board or by email each day in class
You must bring a wifi laptop or tablet for in-class testing
NO FOOD or drink cups can be visible during lab/Chairs must be UNDER the desk during lab and you must stand/ NO FOOD OR MICROBES IN THE LAB DRAWERS!
The Course Calendar (menu right) will show you approximate dates for major EXAMS, Tests, and Microbiology 40 meetings... please see the Daily Agenda for confirmation each week or see this DAILY ANNOUNCEMENT PAGE - do not contact the admin or Chair if you are confused - EMAIL or text me!
NOTE: This site utilizes Google Drive, a file storage and sharing cloud service. It is not required to have a Google or Google Drive account but will require this soon - it might be best to obtain a gmail account to make things work more seamlessly. Links for access to course material posted to Google Drive can be found on this site.
All course material posted to this site, including the site itself, can be accessed on all desktop browsers including Explorer, Chrome, Firefox, Safari and Opera; as while as their mobile browser counterparts in addition to Skyfire, S60, Dolphin, UC and Blackberry browsers. Please contact Professor Hicks immediately for any problems encountered on your device or browser.
CONTACT INFORMATION
Professor Donald R Hicks (Prof Hicks)
hicksmicro@gmail.com
Dr Felecia Tsang is our Micro Labtech
(323) 953-4000 x 2801They are in SC-110.
MY OFFICE HOURS: Office hours are Sunday Zoom 3-4 PM,1 hour before class (6 PM) or by appointment in Science Building (SCI) 110/112. . Appointments should be made and confirmed by email.
THE LA Sheriff's Office EMERGENCY TELEPHONE NUMBER: 323-662-5276 or from a campus phone press #3; call the LA CITY COLLEGE Sheriff's Office BEFORE 911!
EMAIL RULES
The college supplies each student with a personal, private unique email address, which must be used in all communication. Students who do not receive emails from Professor Hicks during the first or subsequent weeks must check with enrollment personnel in the administration building immediately to verify their correct email address has been provided to the instructor and that they understand how to access and utilize this official email communication service provided by the college. BECAUSE I RECEIVE HUNDREDS OF EMAILS A DAY AND THUS YOUR IMPORTANT COMMUNICATION TO ME MIGHT GET "LOST," use:hicksmicro@gmail.com
All emails must be formatted as requested and include in the SUBJECT LINE:your Last name, first name, your student ID#, followed by a brief topic statement "tag" or "hint." For example, in the subject line, put something like this: Hicks, Donald ID#34456555 Absent illness 7/1/2026
All information wished to be communicated must be written in the body of your email. Also, within the body of your email, state whether an attachment is included with your email. Only "Word" documents will be accepted as attachments. This includes (.doc) and (.docx) file formats.
Do not email questions on test days or the night before any evaluation. They will not be answered as I am preparing the paperwork for the evaluation and lack the time to properly answer late questions.
PAPERS SUBMITTED FOR GRADING
All papers submitted for grading must be typed. All submissions for grading must have the following information PRINTED in the upper right hand corner (or on side 1 of a Scantron in the NAME Box NOT ON THE BACK OF ANY SCANTRON!). Your PRINTED LAST name, printed first name; class name and section number (i.e., M-20 Spring 25), the test/exam form letter and number (i.e., Exam 1A #34) if on a scantron and the date submitted. Besides Scantrons, all other submissions must be typed except the LRB. On the first page place your name, class and section number and the date in the upper right corner of the first page. Pages must be numbered as well. Failure to follow these rules will result in -5 pts for EACH part of the rule omitted on each paper EVERY TIME you submit in error.
LECTURE & LABORATORY RULES & BEHAVIOR
Please be aware that some class lectures, labs, and help sessions are videotaped for teaching purposes and improvement of instructions. By attending, students are consenting their permission to be filmed in a teaching situation.
Students may not enter any microbiology class or lab without the presence of the instructor or department staff. However, students may enter the classroom to wash their hands, disinfect, and seat themselvesifthe door is open. Student class Volunteers may enter to perform PRE-CLASS assignments as well - knock on the door of SC-110 & 112 if the rooms are locked and you arrive early to perform these tasks.
Students may not enter the lecture or lab and work on lab assignments without permission. Lab work may continue during scheduled course times only.
Food and/or drinks are not allowed in or during lab, whatsoever; and no visible cups, bottles, or food containers. Smoking, make-up application, texting, talking on cell phones, sleeping, or any other distracting behavior will also not be tolerated during lecture or lab. While microbes are present on the tables in the laboratory, all students must have their chairs "pushed" under the table-tops and be standing in proper lab attire (lab coats and gloves). If you need to exit the lab, remove your lab attire - DO NOT WALK THE HALLS in lab attire. Note: the outside corridor doors are LOCKED during any active lab (if you are locked outside - knock on the door).
Lab spills should be disinfected immediately and the instructor notified. Glass breakage is NOT to be cleared by students - please spray disinfectant on the breakage and contact the instructor for assistance in cleaning.
VOLUNTEERS are sought for those wanting COURSE BONUS POINTS who would like to perform before or after class duties, see CLASS POINTS ABOVE.
*PLEASE treat everyone with respect and courtesy. Each and every student is expected to display equal and proper respect to others. Please avoid any overt or perceived actions that may be interpreted as prejudice or discrimination, including but not limited to discrimination based on age, sex, religion, race, ethnicity, disability, sexual orientation, or economic status. Such behavior will be grounds for immediate dismissal from class, pending administrative review.
CHEATING/TESTING: During all class evaluations, you will be seated randomly, and your personal items are to be placed under or on the teacher tables at the front of the room - DO NOT LEAVE ITEMS IN THE WALKWAYS - place them on or under the tables. Instructions/Test Direction for each test will be found on each test. Failure to read these directions in their entirety may cause the loss of potential test points.To ensure students review this site daily, as required, tests will contain questions pertaining to the navigation of this site. Evaluations, including pop quizzes, will cover material discussed or assigned from the first to the last lecture day before the test. Please be aware that material in class will not follow the textbook, and some lectures may incorporate material from a variety of chapters throughout the textbook, or from material found on handouts and videos.
Talking, whispering, cheat sheets, taking test question sheets out of the classroom, photographing tests, using phones and other electronic devices, changing graded answers, using false data, copying without referencing the source, copying another person's work, or exchanging different "forms" of a test during its administration is grounds for a zero (0) grade. If you received a (0), it is not because of an error. If you have a question about a grade, contact me by email or in class. If you have a question during an evaluation, raise your hand at that moment and then come and ask me quietly for the required information. Do not photograph exam question sheets without first obtaining permission. Do not ask for a bathroom break or any other "break" during evaluations - only in extreme emergencies will such a request be allowed, and those permitted shall leave their cell phone or other communication device in the classroom and be accompanied by a monitor.
Upon the belief of cheating, you will be asked to leave the class evaluation, and evidence, including witness statements, will be collected. Subsequently, you will be contacted for a meeting to discuss the event with the instructor and the Dept. Head, which could result in a charge of Academic Dishonesty by the college. Cheating on a required component of the course will result in the assignment of an (F) grade in the course. Since you are training to become healthcare workers,I take cheating very, very seriously.PLEASE DO NOT CHEAT! If you have a problem, contact me before testing - contact me immediately - and I will do anything I can to help you succeed in the class!
ELECTRONIC DEVICES: All electronic devices must be turned off or set to vibrate before entering the classroom & placed face down on your table-top. YOU MAY NOT TEXT, SURF, or EMAIL DURING LECTURE OR LAB.However, you may quietly leave the room (and return) if you have an emergency situation or contact. Students may voice-record lectures or use a laptop to take notes. Outside of the Microbiology business, emailing, texting, or chatting is not permitted on any device used during class lecture or laboratory.
10 Steps to an easy "A" in Microbiology:
(1) attend EVERY class, including every ZOOM Help, Extra Lab Practice, and Exam Review Session
(2) READ the assigned material in the textbook online (microdropbox link) or in an old edition & in the notes the night BEFORE each lecture
(3) PRINT out the notes and bring them to class; fill in any information not in the notes; ASK questions during lecture
(4) FORM a study group of 3-5 that meets weekly and reviews and discusses the notes and OLD TEST QUESTIONS.
(5) During testing, READ every test question completely as there may be more than 1 correct answer (6) REVIEW any questions you miss on any test/evaluation and determine "why" you missed the question - the correct answer for each marked wrong is listed in RED (if you still do not understand WHY, ask me)
(7) VOLUNTEER to be a class checker for BONUS POINTS!
(8) DO ALL the CLASS-WIDE BONUS POINT assignments on time and do them perfectly; do each evaluation BONUS POINT section (they are: in the Lab Record Book - your video notes of each assigned video, the class agenda, the Library Assignment, and the Parasite Assignment)
(9) REVIEW the most missed questions and any new material covered in class for the Comprehensive Final Exam
(10) Prepare your formal typed Unknown Report in advance by coming to the ZOOM Unknown Report Review Session and turning it in on the last class day before the Final for PRE-GRADING (guaranteed 90% if complete & only a 10 errors
Students will receive one (1) warning about inappropriate use and setting(s) of their electronic devices. Further failure to observe course rules regarding electronic devices will cost the offending student ten (-10) points per offense on that or the next evaluation.
Students are expected to come prepared to any evaluation with a good #2 pencil with eraser; I supply the Scantrons. Those who wish to change an answer may erase, remark, and place a capital letter of their new answer over the letter (G) of their "Scantron".
Students will be dropped if two (2) complete class meetings are missed without an approved written excuse. Those who received an (I) in a previous term and are repeating or making up the course should not re-register, but discuss with Professor Hicks which class they are going to attend with Professor Hicks. REMEMBER, After one (1) calendar year, a grade of (I) will default to the grade listed on the received academic notification, usually an (F) grade.
*Your final average and final class grade is assigned by a computer - NOT BY ME. No one will receive any points outside those provided to each other student equally - DO NOT attempt to "mine" me for extra points. You will receive a MICROGRADESHEET to your official college email within 7-10 days after every evaluation - these become "official" within one week. Check your gradesheets and contact me immediately if you suspect a discrepancy. After 1 week, these grade sheets become official college gradebooks and are not alterable.
When completing all submitted material, PRINT YOUR LAST NAME FIRST, then your first name, Class # and section # followed by your evaluation form LETTER and NUMBER. Place the DATE taken in the space provided – ANY DEVIATION IN THIS WILL RESULT IN -5 to 10 Pts for each error each time. ALL GRADES are FINAL 1 week after any GRADESHEET is distributed. PLEASE discuss any questions about grading PROMPTLY – DO NOT WAIT UNTIL IT IS TOO LATE! NOTE at the end of the term in the Final Exam Packet 1 (ONE) point deduction will be RETURNED TO YOU if you didn't ever do that recording error again. This does not apply to BONUS points.
LECTURE & LAB SEATING/Daily Procedures
Official class seating will be assigned at the conclusion of the second (2nd) week of the term. All seating for lectures and lab is by alphabetical order according to last name. Each class day, students are to leave their belongings in their assigned chairs, wash their hands (well) at the sink, and wipe down the tabletop with the provided disinfectant before touching the tabletops. Please use the same paper used to dry hands to smear the disinfectant around the tabletop and let it air-dry. Before exiting the lab, students are to complete these actions in reverse. Please do not leave the lab wearing smocks and/or gloves on, as it "frightens the natives in the halls." When microbes are present, students must be in lab attire (lab coats + gloves) and the chairs are to be "pushed" under the table tops (put your things in the chairs), the room doors are locked, and the tabletops are disinfected with only the LRB and or lab materials left available on top for student use.
FINAL EXAMINATIONS
Spring 2026 are as listed by LACC & is usually the 1st Tuesday night of Final Exam Week
TEST ERRORS: I don't curve. I do put BONUS questions on every test. If there is a misgrade on your test, NO MORE THAN 4 mis-erasers 2X during any term will be re-applied to your grade. Learn to mark carefully. When I see cheating, I take witness statements as well as the "Proctor's" statement... Then, I apply the consequences. If you wish to challenge this, please make an appointment by email!
Beginning in Week 3, the VOLUNTEER Checkers should do the scopes before and after class, and the Room/Sink Checkers should check the room, clean the sinks, and refill the stains, lens paper containers, and disinfectant bottles each day! IF YOU ARE A "CHECKER," have me SIGN your LRB during the LAST week of the term - AFTER you have done your assignment!
Please don't email questions that can be found by viewing this INDEX PAGE! Or if you have not copied the board agenda daily - LOOK IN YOUR LRB or here. If the dates/info are in CONFLICT, the MASS EMAIL "trumps all" followed by the INDEX PAGE. Why? Because individual classes may move faster or slower than our planned daily agenda accounts for...
ALL SCANTRON TESTS are graded ASAP, and Grade sheets are returned/updated about every month near the 1st... check your email. If you find an error on your SCANTRON or GRADESHEET, circle the scantron number in RED pen and return it to me ASAP. If the error is on your gradesheet, print out the gradesheet and circle the error in RED and bring it to me in your next class... NOTE: All scantrons/essays/evaluation materials are SCANNED by me before I return them to you for review and consideration for the Final Exam. DO NOT ALTER ANY SUBMITTED MATERIAL as they are checked for alterations. Any "bogus" changes/faked errors will result in a dishonesty measure (grade recorded as a "0"
HOW TO BEGIN ORGANIZING FOR A NEW TERM!
Over the years, I have added several things to the class besides the usual textbook, lecture, and lab exercises. The first was to delete the cost and waste of a lab manual (you print your own using the Microwebsite/microblogsite) and the design of a class website. The Microblogsite assists you in obtaining copies of many class materials that you might not normally be able to access. I have added many other features and ancillary materials since, and more are to come.
Remember, the assistance provided below is NOT REQUIRED of me; I do it because I want YOU to do well in the class and to make it easier and more adaptable to the changing requirements of Science. HOWEVER, I am not a computer designer/engineer, and my learning curve is steep. Things may not work perfectly for everyone or anyone, and alterations may be needed instantly to make our ideas/technology work or continue to work. Try, ask, be flexible, and it will help us all!
IMPORTANT:The MICRODROPBOX link below contains several important ancillary materials, including video lectures, audio lectures, copies of old test questions, helpful study charts, old editions of texts, and the class PowerPoint presentations.
Here are the resources I have designed and/or provided:
(1) Class notes from the outlines/Pdf's/PowerPoints used in lecture (2) Instructions on how to do the labs and what they teach, as well as what things "look like." (3) Chat on Zoom or the Class text number (4) Copies of MY old test questions that you can use - NOT FOR MEMORIZATION, but to check your progress and to learn HOW I ask questions on exams - (5) Videos of the lecture material and labs - MICROBLOGSITE UTUBE LIST (6) NEW material -- as SCIENCE changes by the minute (7) NEW teaching/electronic media presentations, as this is also changing almost daily! (8) Example Term Papers and assistance with writing the required class term paper - MICROBLOGSITE BUTTON (9) Forums/discussion sites for interaction and solutions of hardware/software problems - Microwebsite from our Zoom (10) A monthly email of your current GRADES on a privately emailed gradesheet... (11) Instant email notice of changes/concerns/announcements - MASS CLASS EMAIL (12) A student email address dedicated ONLY to students, which is monitored constantly!
RE-GAINING minus points taken on any 1 test or exam - GRADING ON "FAILURE TO FOLLOW TEST DIRECTIONS": You can return one (1) paper that I have taken off points for recording infractions once by putting it in your Final Exam packet, and I will give them back ONCE on 1 paper only! I will NOT return points for cheating or writing on exams. I WILL NOT MAKE CORRECTIONS ON SCANTRON ERASERS MORE THAN up to 4 erasers on 1 paper per term! If you do not buy a better eraser and learn to erase and remark.. You will have to retake the exam using a different version of the exam. No more than 4 erasers on 1 test ONCE. If there is another dispute, you may request to retake another version of the Exam after the second instance of "misgrades."
STUDENT LEARNING OUTCOMES:
On the "answers" for the OLD LP1 TESTS/Exam questions- NO! I don't have the answer sheets... this is college not kinder garden! I don't do the work, you do. You are NOT supposed to memorize but reason... So, HOW do I study? GET TOGETHER IN A STUDYGROUP AND "WORKOUT/DISCUSS" each question and understand WHY? I wrote it.
*IMPORTANT COMMENTS:Save theMICRODROPBOX link as it contains a number of important ancillary materials including video lectures, audio lectures, copies of old test questions, helpful study charts, old editions of texts, as well as the class POWERPOINTS.
NOTE! If you miss 2 classes without an approved excuse you will be dropped! TESTS ARE RETURNED ABOUT 1 WEEK AFTER Administration! GRADESHEETS are EMAILED to your official college email address about 10 days after each grade is earned/changed. Microbiology Labs are kept very very coldto lower bacterial growth, counter the effects of 30 lighted Bunsen Burners, and to lower the chance of bacterial contamination - you may want to wear warmer clothing or a lab coat during lecture. Clickable Links look like this or with buttons on this website (if you click here you will return HERE)! Clickable links on the Microblogsite are YELLOW or are in a clickable button. WASH your hands and Disinfect your tabletop FIRST & DAILY!
Global Virus Forecasting: http://www.gvfi.org/ Find out for yourself! You may want to explain why we let this happen to your children... Publications where you can read the evidence: http://www.gvfi.org/publications.php
ADDITIONALLY after reading this HOME or INDEX PAGE -
Then, go to the right-hand menus and review each of them...
Finally, click on Microdropbox link and EXPLORE IT!
INCOMPLETES:If you received an incomplete (i) in microbiology for ANY term, you must attend the first day of one of my classes for the NEXT term. You have 1 yr to finish the class. When you arrive, notify me immediately that you are making up an Incomplete. Pick the one of my classes that best fits your schedule to attend. If you do NOT do this the Incomplete reverts to the second grade listed on your Grade Report.
If you made up a previous Incomplete during a previous semester, the new grade will not appear on your transcript for about 4 weeks, if is doesn't, contact me.
DO NOT GET BEHIND; especially recording your LRB BONUS POINT video notes! If a video is listed on the daily agenda then it is assigned for viewing and must be "noted" front to back in your LRB with a * LAB HINTS!
FOR EACH EXPERIMENT IN LABORATORY AND LECTURE - YOU NEED TO UNDERSTAND "THESE USAGE/vocabulary TERMS concerning the Experiments/Tests we are likely to perform:" Chemistry (found in the Atlas and or on the website in the 1st or second paragraph of each page) Inoculation(according to media: broth (loop-dip), slant (loop zig-zag), deep (needle stab), slant-deep (needle stab + loop zig-zag, plate - melt pour cool and loop line shared) Incubation(at Opt. Temp. Test; for 7 days checking every-other day (color change by itself) or for 7 days and test for tests with drops) Evaluation (in the Atlas and on the Webpage) CAUTIONS/COMMENTS (usually in lecture and on the Webpage) EXPLANATION of the TERMS USED ABOVE: CHEMISTRY - This material explains the chemical basis of the test (What are we testing for?) and is usually found both in the M20 Laboratory Guide, Atlas and online...
INOCULATION - this is a brief description of how you place your microbe into the test medium... There are 5 main ways of inoculation: (1) LOOP DIP a BROTH- you heat and cool your loop, scoop-up a small amount of your microbe, and then put the loop just below the surface of the test broth or liquid. You do NOT "bang it" or try and remove the microbe from the loop - just "dip it!"Then, you heat and cool the loop and put it away. (2) LOOP ZIGZAG on a SLANT - you heat and cool your loop, scoop-up a small amount of your microbe, and then put the loop at the back end of a test tube containing a slant of agar and (in a zigzag pattern; or in a straight 4cm line on one side of an agar plate) you pull it forward to the tip of the slant. You do NOT "bang it" or try and remove the microbe from the loop!"Then, you heat and cool the loop and put it away. (3) LOOP "LINE" SHARED on an AGAR PLATE TEST - you heat and cool your loop and scoop-up a small amount of your microbe and put a 2.5 cm or 1 inch line as far away as possible from your lab partner on a cooled agar plate (label your line with a Sharpee on the underside of the plate). Then heat and cool your loop and put it away. (4) NEEDLE STAB on an AGAR DEEP - you heat and cool your needle, scoop-up a very small amount of your microbe (DON'T TEAR THE AGAR!!!) and then smoothly stab the needle 3/4 down the center of an agar filled deep or slant-deep making sure to go in and out of the SAME hole. You heat and cool the needle and then put it away. (5) LOOP ZIG-ZAG SLANT/NEEDLE STAB DEEP on a SLANT/DEEP TEST - you do both the Loop Zigzag and a Needle Stab on the same tube (this tube is NOT as slanted as a normal slant and is known as a SLANT-DEEP).
INCUBATION- This is the process of "cooking" your test microbe inside the test media. The temperature is determined by your OPTIMUM TEMPERATURE TEST. EVERY CARD HAS this statement "you use the temperature for incubation as determined by your Optimum Temperature Procedure." The amount of time in the incubator is determined by the type of test and your schedule. It is best to check every-other day...but, if that is not possible - then, check each class period. A good general rule to follow is this... There are 3 incubation times: (1) some tests are incubated just 48 hours and then reagents are added and the test is mixed, read, recorded and discarded... or the test media turns a color and it is read, recorded and discarded. (2) If DROPS/REAGENTS are added after incubation, then these tests are incubated usually 7 days and the drops are added and the test is mixed, read, recorded and discarded - note these tests are only POS or NEG. & (3) If the test media changes color without adding ANY reagents, then check it for every other day or for 3 labs (7 days) and MIXED WELL, read (re-incubate if negative) recorded, and discarded. If it ever turns the positive color you should record the time and color and discard. If after the first lab it is positive record is as a FAST POSITIVE, if not, return it to the incubator. If after the second lab it is positive, record it as a MODERATELY FAST POSITIVE, if not, return it to the incubator. It after the third lab, it turns the positive color, then record it as a SLOW POSITIVE. If it never turns the positive color and at least 3 labs have past, discard and record it as a NEGATIVE. Remember to remove all tape and marks from discarded tubes and plates and place small tubes in the small discard rack at an angle... large tubes go in the large discard rack!
EVALUATION- This is the process of recording the results of the test. If the test must change color without any reagents being added follow the instructions above in INCUBATION. If the test must have some solution(s) added to it to see if it is positive, then leave it in the incubator for a total of 3 labs, take it out, mix it, add the solutions in the correct order, mix it again and let it set for at least 10 minutes before making a negative decision. If the test is the VP TEST, it must incubate for a minimum of 10-14 days and must it must sit overnight after the reagents are added BEFORE a decision is made! Don't forget to list the chemical names of the reagent used in each test - you must know them! Gelatin is re-incubated for up to 21 days if negative when read each lab.
CAUTIONS/COMMENTS- Some tests have specific problems brought out in the online discussion... list them here. For example, the Thioglycollate Broth test must NOT BE SHAKEN or disturbed during inoculation and incubation...
Look for the information during the term concerning the FE BONUS Short Answer Essays - everyone will be assigned 1 of 3 at random...
(1) Explain Hep C treatment (interferon/Ribavirin yes or no - why & why its curable; what strains and how long;
(2) What is "Truvada Prophylaxis" & why is LA County in an experiment to triple attack new HIV infections (bottom of this page); how might it stop the spread of HIV in combo with HIV treatment; or
(3) Discuss “AIDS Denialism” dispute at least 5 of 13 arguments denialists use & explain why this idea is FAKE SCIENCE/pseudoscience!
PREPARE! GET the BONUS!!
Videos on FE:Herpes: the Invasive Invader, And the Band Played On, TED Viral Chatter video 1st video:TED Zoonosis Viral Chatter video (CLICK HERE)1st video:,Hep C, The War on HIV, AIDSVAX 60 Min 2, readings on Truvada at the bottom of this page - go very far down... SEE THE REST UNDER PART 3 EXAM 3!
AIDS DENIALISM arguments Debunked - Its the best example of FAKE Science Pseudoscience! FE Bonus!
Technicians hold up a bag of modified T cells genetically edited to resist HIV infection. (Credit: Penn)
June and his colleagues, including Bruce L. Levine, professor in cancer gene therapy and the director of the Clinical Cell and Vaccine Production Facility at Penn, used zinc finger nuclease (ZFN) technology to modify the T cells in the patients—a “molecular scissors,” of sorts, to mimic the CCR5-delta-32 mutation.
That rare mutation is of interest because it provides a natural resistance to the virus, but in only one percent of the general population. By inducing the mutations, the scientists reduced the expression of CCR5 surface proteins. Without those, HIV cannot enter, rendering the patients’ cells resistant to infection.
T CELL INFUSIONS
For the study, the team infused the modified cells –known as SB-728-T—into two cohorts of patients, all treated with single infusions—about 10 billion cells—between May 2009 and July 2012. Six were taken off antiretroviral therapy altogether for up to 12 weeks, beginning four weeks after infusion, while six patients remained on treatment.
Infusions were deemed safe and tolerable, the authors report, and modified T cells continued to persist in the patients during follow up visits. One week after the initial infusion, testing revealed a dramatic spike in modified T cells inside the patients’ bodies. While those cells declined over a number of weeks in the blood, the decrease of modified cells was significantly less than that of unmodified T cells during ADT treatment interruption.
Modified cells were also observed in the gut-associated lymphoid tissue, which is a major reservoir of immune cells and a critical reservoir of HIV infection, suggesting that the modified cells are functioning and trafficking normally in the body.
The study also shows promise in the approach’s ability to suppress the virus. The viral loads (HIV-RNA) dropped in four patients whose treatment was interrupted for 12 weeks. One of those patients’ viral loads dropped below the limit of detection; interestingly, it was later discovered that the patient was found to be heterozygous for the CCR5 delta-32 gene mutation.
“Since half the subject’s CCR5 genes were naturally disrupted, the gene editing approach was building on the head start provided by inheriting the mutation from one parent,” says Levine. “This case gives us a better understanding of the mutation and the body’s response to the therapy, opening up another door for study.”
PROTECT THE T CELLS
Therapies based on the CCR5 mutation have gained steam over the last six years, particularly after a man known as the Berlin Patient was “functionally” cured. Diagnosed with acute myeloid leukemia (AML), he received a stem cell transplant from a donor who had the CCR5 mutation in both alleles (from both parents) and has remained off ADT since 2008.
Researchers are attempting to replicate this phenomenon because allogeneic transplants—which carry a high mortality risk and require lengthy hospitalizations—are not a practical solution for HIV patients who do not have blood cancers. Nor are they effective in ridding the body of HIV unless the donor has the mutated gene in both alleles, as shown recently in two Boston patients who were thought to have been “functionally” cured from transplants, only to see their viral loads spike.
Though disappointing to the research community, the Boston patients’ results highlight key factors when combating the virus.
“Those cases emphasize the need to protect T cells from the virus,” says Pablo Tebas, director of the AIDS Clinical Trials Unit at the Penn Center for AIDS Research, one of two centers where the study was completed.
“The Boston cases show us that for the Berlin patient, it was not the chemotherapy or infusion of a donor’s stem cells that staved off the HIV; it was the protection of the T cells by the lack of CCR5. Those procedures couldn’t completely eliminate the reservoir of the HIV virus, and when the virus came back the T cells were susceptible to infection. The ZFN approach protects T cells from HIV and may be able to almost completely deplete the virus, as those cells are still functional.”
Further clinical trials will evaluate greater numbers of modified T cells in a larger cohort of patients, as well as strategies to increase the persistence of more cells in the body to achieve a therapeutic effect.
A NIAID Program Project Grant, the Penn Center for AIDS Research, Clinical Trials Unit, and Sangamo BioSciences funded the study.
Additional researchers at Penn Medicine, the Albert Einstein College of Medicine, and scientists from Sangamo BioSciences, which developed the zinc finger nuclease (ZFN) technology, the T cell therapy approach used in the clinical trial, co-authored the phase I study.
Patients seeking information about Penn Medicine’s gene therapy trials for HIV can call Joe Quinn in the AIDS Clinical Trials Unit
*HOW IS TRUVADA USEDTO TREAT HIV-1 INFECTION
Truvadais a type of medicine called a nucleoside analog reverse transcriptase inhibitor (NRTI) that is used to treat HIV-1 infection in adults and teenagers (12 and older).
TRUVADA is a combination therapy because it has 2 medicines in 1 pill– emtricitabine and tenofovir disoproxil fumarate. TRUVADA is always used with other anti-HIV medicines to treat HIV-1 infection because TRUVADA alone is not a complete treatment.
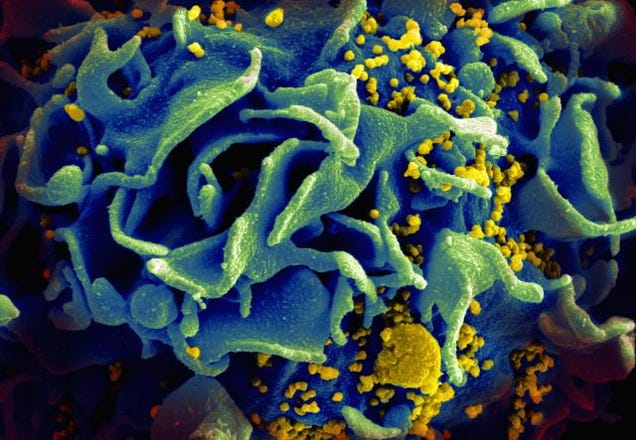
Understanding HIV
HIV infects important cells for fighting infection called CD4 cells, or T cells. Once HIV enters the body, the virus multiplies inside these cells. These new viruses are released into the blood and infect other CD4 cells.
How TRUVADA/DESCOVY can help
When used with another anti-HIV-1 medicine, TRUVADA helps make it harder for HIV-1 to multiply by blocking an enzyme in your body called reverse transcriptase
By helping to keep HIV-1 from multiplying in your body, TRUVADA helps lower the viral load, which means decreasing the amount of HIV in the blood
TRUVADA may also help increase the number of CD4 cells when used with another anti-HIV-1 medicine
TRUVADA is a prescription medicine used in 2 different ways:
to treat HIV-1 infection in adults and teenagers (12 and older). When used for the treatment of HIV-1 infection, TRUVADA is always used together with other HIV-1 medicines.
to help reduce the risk of getting HIV-1 infection when used together with safer sex practices. This use is only for adults who are at a high risk of getting HIV-1. This includes HIV-negative men who have sex with men and who are at high risk of getting infected with HIV-1 through sex, and male-female sex partners when one partner has HIV-1 and the other does not.
TRUVADA does not cure HIV-1 infection or AIDS. Ask your healthcare provider if you have questions about how to prevent getting HIV-1 or passing HIV-1 to others. Always practice safer sex and use condoms to lower the chance of sexual contact with body fluids. Never reuse or share needles or other items that have body fluids on them. If you are taking TRUVADA with other HIV-1 medicines to treat HIV-1, you must keep taking TRUVADA to control HIV-1 infection and decrease HIV-1 related illnesses.
IMPORTANT SAFETY INFORMATION
What is the most important information I should know about TRUVADA?
TRUVADA can cause serious side effects:
Too much lactic acid in your blood (lactic acidosis), which is a serious medical emergency. Symptoms of lactic acidosis include weakness or being more tired than usual, unusual muscle pain, being short of breath or fast breathing, nausea, vomiting, stomach-area pain, cold or blue hands and feet, feeling dizzy or lightheaded, and/or fast or abnormal heartbeats.
Serious liver problems. Your liver may become large and tender, and you may develop fat in your liver. Symptoms of liver problems include your skin or the white part of your eyes turns yellow, dark “tea-colored” urine, light-colored stools, loss of appetite for several days or longer, nausea, and/or stomach-area pain.
You may be more likely to get lactic acidosis or serious liver problems if you are female, very overweight (obese), or have been taking TRUVADA for a long time. In some cases, these serious conditions have led to death. Call your healthcare provider right away if you have any symptoms of these conditions.
Worsening of hepatitis B (HBV) infection. If you also have HBV and take TRUVADA, your hepatitis may become worse if you stop taking TRUVADA. Do not stop taking TRUVADA without first talking to your healthcare provider. If your healthcare provider tells you to stop taking TRUVADA, they will need to watch you closely for several months to monitor your health. TRUVADA is not approved for the treatment of HBV.
If your healthcare provider has prescribed TRUVADA to help reduce the risk of getting HIV-1 infection, you should also know:
You must be HIV-negative before you start taking TRUVADA to reduce the risk of getting HIV-1. You must get tested to make sure that you do not already have HIV-1 infection. Do not take TRUVADA to reduce the risk of getting HIV-1 unless you are confirmed to be HIV-negative.
Many HIV-1 tests can miss HIV-1 infection in a person who has recently become infected. If you have flu-like symptoms, you could have recently become infected with HIV-1. Tell your healthcare provider if you had a flu-like illness within the last month before starting TRUVADA or at any time while taking TRUVADA. Symptoms of new HIV-1 infection include tiredness, fever, joint or muscle aches, headache, sore throat, vomiting, diarrhea, rash, night sweats, and/or enlarged lymph nodes in the neck or groin.
Just taking TRUVADA may not keep you from getting HIV-1. You must continue using safer sex practices while you are taking TRUVADA to reduce your risk of getting HIV-1. To further reduce your risk of getting HIV-1:
Get tested for other sexually transmitted infections. Other infections make it easier for HIV-1 to infect you.
Get information and support to help reduce risky sexual behavior.
Have fewer sex partners.
Do not miss any doses of TRUVADA. Missing doses may increase your risk of getting HIV-1 infection.
You must stay HIV-negative to keep taking TRUVADA to reduce your risk of getting HIV-1:
Know your HIV-1 status and the HIV-1 status of your partners.
Get tested for HIV-1 at least every 3 months or when your healthcare provider tells you.
If you think you were exposed to HIV-1, tell your healthcare provider right away.
If you do become HIV-1 positive, you need more medicine than TRUVADA alone to treat HIV-1. TRUVADA itself is not a complete treatment for HIV-1.
If you have HIV-1 and take only TRUVADA, your HIV-1 may become harder to treat.
If your healthcare provider has prescribed TRUVADA to help reduce the risk of getting HIV-1 infection, do not take TRUVADA if:
You already have HIV-1 infection or if you do not know your HIV-1 infection status. If you are HIV-1 positive, you need to take other medicines with TRUVADA to treat HIV-1. TRUVADA itself is not a complete treatment for HIV-1. If you have HIV-1 and take only TRUVADA, your HIV-1 may become harder to treat.
What are the other possible side effects of TRUVADA?
Serious side effects of TRUVADA may also include:
New or worsening kidney problems, including kidney failure. Your healthcare provider may do blood tests to check your kidneys before and during treatment with TRUVADA. If you develop kidney problems, your healthcare provider may tell you to take TRUVADA less often, or to stop taking TRUVADA.
Bone problems, including bone pain or bones getting soft or thin, which may lead to fractures. Your healthcare provider may do tests to check your bones.
Changes in body fat can happen in people taking HIV-1 medicines.
Changes in your immune system. If you have HIV-1 infection and start taking HIV-1 medicines, your immune system may get stronger and begin to fight infections. This may cause minor symptoms such as fever, but can also lead to serious problems. Tell your healthcare provider if you have any new symptoms after you start taking TRUVADA.
The most common side effects of TRUVADA are:
In people taking TRUVADA with other HIV-1 medicines to treat HIV-1 infection, common side effects include: diarrhea, nausea, tiredness, headache, dizziness, depression, problems sleeping, abnormal dreams, and rash.
In people taking TRUVADA to reduce the risk of getting HIV-1 infection, common side effects include: headache, stomach-area (abdomen) pain, and decreased weight.
Tell your healthcare provider if you have any side effects that bother you or don’t go away.
What should I tell my healthcare provider before taking TRUVADA?
All your health problems. Be sure to tell your healthcare provider if you have or had any kidney, bone, or liver problems, including hepatitis virus infection.
If you are pregnant or plan to become pregnant. It is not known if TRUVADA can harm your unborn baby. Tell your healthcare provider if you become pregnant while taking TRUVADA. If you are taking TRUVADA to reduce the risk of getting HIV-1 and you become pregnant, talk to your healthcare provider to decide if you should keep taking TRUVADA.
If you are breastfeeding (nursing) or plan to breastfeed. Do not breastfeed. HIV-1 can be passed to the baby in breast milk. Also, the medicines in TRUVADA can pass into breast milk, and it is not known if the medicines can harm the baby.
All the medicines you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements. TRUVADA may interact with other medicines. Keep a list of all your medicines and show it to your healthcare provider and pharmacist when you get a new medicine.
Your healthcare provider may need to check you more often or change your dose if you take any of these medicines with TRUVADA: didanosine (Videx EC), atazanavir (Reyataz), darunavir (Prezista), or lopinavir with ritonavir (Kaletra).
You are encouraged to report negative side effects of prescription drugs to the FDA. Visit www.FDA.gov/medwatch, or call 1-800-FDA-1088.
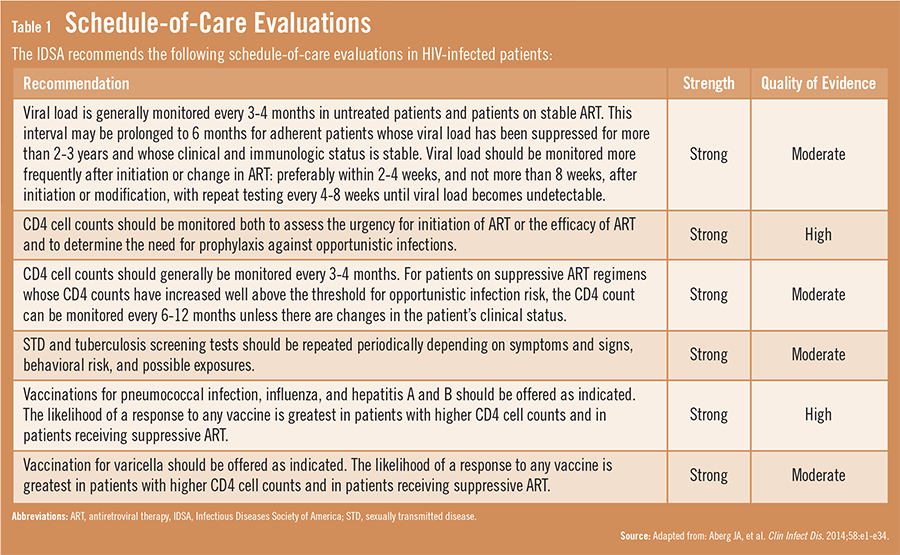
Guidelines have been updated to reflect the fact that people with HIV are now living normal life spans. In addition to routine HIV management, the guidelines emphasize that clinicians focus on preventive care for other serious health conditions.
According to the CDC, nearly 1.2 million Ameri-cans are living with HIV and about 50,000 people in the United States are infected with the virus each year. Studies have estimated that as many as 80% of patients with HIV have their virus under control and live long, full lives. “With HIV continuing to become a manageable but complex chronic disease, HIV specialists and primary care physicians (PCPs) now need to provide the full spectrum of healthcare to these patients,” says Michael A. Horberg, MD, MAS, FACP, FIDSA. “PCPs and other healthcare providers need a better grasp of the impact that HIV care has on routine healthcare.”
A Helpful Update
In 2009, an expert panel of the HIV Medicine Association of the Infectious Diseases Society of America (IDSA) released evidence-based guidelines for the management of people infected with HIV. Recently, these guidelines were updated to replace the 2009 recommendations and published in Clinical Infectious Diseases. Since 2009, new antiretroviral drugs and classes have become available, and the prognosis of people with HIV infection continues to improve. The guideline update also incorporates new information based on publications from 2009 to 2013.
“The updated IDSA guidelines are intended for use by healthcare providers who care for HIV-infected patients,” says Dr. Horberg, who was on the expert panel that developed the update. “These new recommendations reflect the fact that people with HIV are now living much more normal life spans. As such, there is a greater need to focus on preventive care, including screening for high cholesterol, diabetes, osteoporosis, depression, and substance abuse, among other health conditions.”
Although there are better survival rates, people with HIV are increasingly developing common health problems that also affect the general population. Some of these conditions may be related to HIV infection itself or its treatment. “An important theme of the guidelines is that HIV-infected patients be managed and monitored for all relevant age- and sex-specific health problems,” Dr. Horberg says.
Summarizing Key Changes
The guidelines have expanded recommendations on the initial evaluation and immediate follow-up for HIV-infected patients. Patients whose infection is under control for some time can have their HIV blood levels monitored every 6 to 12 months, rather than every 3 to 4 months as previously recommended (Table 1). In addition, the guidelines include new recommendations on screening for diabetes, osteoporosis, and colon cancer. They also suggest that patients with HIV infection be vaccinated against pneumococcal infection, influenza, varicella, and hepatitis A and B. “HIV may be under control in many patients, but we still should stress the importance of preventing other health problems,” adds Dr. Horberg. “This requires taking a holistic approach to care.”
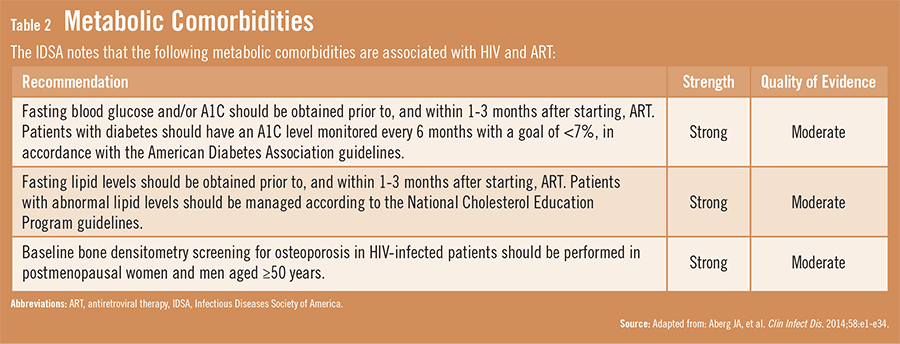
The IDSA’s guideline update has added easy-to-use tables that outline interactions between specific antiretroviral drugs and statins. Importantly, a new section on metabolic comorbidities was added to the guidelines, replacing the need for separate recommendations on dyslipidemia, which had been previously published (Table 2). There also is a more robust section on sexually transmitted diseases, including a recommendation for annual screening of trichomoniasis in women and yearly screening for gonorrhea and chlamydia for patients considered to be at risk.
Behavior Matters
“The guidelines stress that physicians should consistently discuss and counsel patients on their sexual history and any risky behaviors, such as using illicit drugs,” Dr. Horberg says. “We need to do this in a non-judgmental manner. We also need to determine how well patients are coping with living with HIV and if they have a sufficient support network.” General messages about risk reduction should be provided at all healthcare encounters—regardless of risk behaviors—by providers, others in healthcare, or with educational materials (eg, pamphlets, posters, and videos). Tailored messages are critical, especially for patients persistently reporting high-risk behaviors. Referrals to programs capable of offering more extensive interventions are also important.
When HIV is under control, patients often feel that they do not need to see their physicians regularly. Dr. Horberg says adherence is about more than just taking HIV medications on a regular basis. “It’s also about receiving regular primary care,” he says. “HIV specialists and PCPs alike need to be familiar with these issues so that we can bridge treatment gaps in HIV care. These guidelines are designed to help ensure that patients with HIV live long and healthy lives. Hopefully, we can learn more about methods for further enhancing our ability to take a holistic approach to caring for patients infected with HIV.”
Additional Resources:
Aberg JA, Gallant JE, Ghanem KG, Emmanuel P, Zingman BS, Horberg MA. Primary care guidelines for the management of persons infected with HIV: 2013 update by the HIV Medicine Association of the Infectious Diseases Society of America. Clin Infect Dis. 2013 Nov 14 [Epub ahead of print].
AIDSinfo. Guidelines for prevention and treatment of opportunistic infections in HIV-infected adults and adolescents, 2013. Available at: http://aidsinfo.nih.gov/guidelines/.
Dube MP, Stein JH, Aberg JA, et al. Guidelines for the evaluation and management of dyslipidemia in human immunodeficiency virus (HIV)–infected adults receiving antiretroviral therapy: recommendations of the HIV Medical Association of the Infectious Diseases Society of America and the Adult AIDS Clinical Trials Group. Clin Infect Dis. 2003;37:613-627.
Aberg JA, Kaplan JE, Libman H, et al. Primary care guidelines for the management of persons infected with human immunodeficiency virus: 2009 update by the HIV Medicine Association of the Infectious Diseases Society of America. Clin Infect Dis. 2009;49:651-681.
- See more at: http://www.physiciansweekly.com/hiv-guidelines-2013/?utm_source=Physician%27s+Weekly+eNewsletter&utm_campaign=f7afe2e8ab-ID_Hospitalists_CC_Cubicin-3_25_14&utm_medium=email&utm_term=0_35606603ab-f7afe2e8ab-108543397#sthash.Iovy7ctr.dpuf
Studies Cement Value!
Anti-HIV pills, daily or 'on-demand,' work just the same
An international team of researchers has traced the "epidemic ignition" of HIV/AIDS to 1920s Kinshasa, what is now the capital city of the Democratic Republic of the Congo.
Research findings published in the latest issue of Science trace the origins of the outbreak to Kinshasa in the 1920s, where epidemiologists believe it emerged from a "perfect storm" of explosive population growth, a booming sex industry, burgeoning public transportation networks, and the use of unsterilized needles in health clinics. Here's The Guardian's Ian Sample:
An international team of scientists led by the universities of Oxford in Britain and Leuven in Belgium reconstructed the history of the HIV pandemic using historical records and DNA samples of the virus dating back to the late 1950s. The DNA allowed them to draw up a family tree of the virus that traced its ancestry through time and space. Using statistical models they could push farther back than the 1950s and locate the origin of the pandemic in 1920s Kinshasa.
People with HIV in central Africa at the time did not have specific symptoms that would have been written down in their medical records. The virus causes the immune system to collapse, leaving people open to all manner of infections. "For an epidemic like HIV where we're trying to track back to before it was even discovered, genetics is the only source of information we have," said Oliver Pybus, an evolutionary biologist at Oxford University and senior author on the study.
The genetic data suggests that pandemic HIV spread rapidly through the Democratic Republic of the Congo, a country the size of western Europe. From the late 1930s to the early 1950s, the virus spread by rail and river to Mbuji-Mayi and Lubumbashi in the south and Kisangani in the north. There the virus took hold and formed secondary reservoirs from where it spread to countries in southern and eastern Africa.
To be clear: The AIDS virus is believed to have spilled over into the human population years before it gained purchase in Kinshasa, but conditions there were such that the infection was first able to proliferate and spread. It did so quietly at first, stealing its steady way through the surrounding area for several decades before thundering, deadly and swift, across the globe.
by Michael Smith North American Correspondent, MedPage Today
Action Points
A vaccine against hepatitis E (HEV) provided protection against the virus for more than 4 years, researchers reported.
In a randomized clinical trial, volunteers getting the HEV vaccine (Hecolin) were significantly less likely to acquire the virus than those getting a control hepatitis B vaccine, according to Ning‑Shao Xia of Xiamen Universityin Xiamen, China, and colleagues.
Over 54 months of follow-up, more than 85% of those who received all three doses of the vaccine maintained antibodies to HEV, Xia and colleagues reported in the New England Journal of Medicine.
HEV is an important cause of acute hepatitis worldwide, the researchers noted, with two distinct epidemiological patterns -- waterborne infection and transmission from animals to humans and among humans.
The waterborne infection, caused by HEV genotypes 1 and 2, primarily takes place in resource-limited areas, while the zoonotic and human-to-human transmission occurs in both developed and developing regions.
One analysis suggested the impact of HEV genotype 1, in regions where the virus is endemic, might be 3.3 million cases yearly, resulting in 70,000 deaths and 3,000 stillbirths, the investigators noted.
In most patients, symptomatic HEV leads to an acute hepatitis that is "indistinguishable from other forms of acute viral hepatitis, is usually self-limited, and does not become chronic," the researchers wrote, except in people with severely compromised immune systems.
On the other hand, disease can be severe in pregnant women, elderly men, and people with pre-existing chronic liver disease, they noted.
The vaccine under study is based on HEV genotype 1 and was licensed in China in 2012, but information on its long-term efficacy wasn't available. To fill the gap, the researchers studied participants in the original 19-month efficacy study for an additional 36 months.
Over the whole study, the researchers found 60 cases of hepatitis E, seven of them in the 53,602-strong vaccine group and 53 among the 53,602 control volunteers who got a hepatitis B vaccine.
Those numbers yielded incidence rates of 0.3 cases and 2.1 cases per 10,000 person-years, respectively, representing a vaccine efficacy of 86.8%, the investigators reported.
Over the trial and extended follow-up, 87% of participants who were seronegative at baseline and who received three doses of the vaccine maintained antibodies against HEV for at least 4.5 years.
Also, HEV antibodies developed in 9% in the control group, they reported.
The investigators reported that the rate of serious adverse events was similar between arms of the study, but none was thought to be related to the study drug.
The vaccine fills a need but it's not clear how large that need is, commented Eyasu Teshale, MD, and John Ward, MD, both of the CDC in Atlanta.
While it's clear that HEV causes death and illness on a large scale in some parts of the world, there is an "absence of precise data regarding the burden of hepatitis E disease and related deaths," they noted in an accompanying editorial.
In particular, there is only limited information on infection during childhood, suggesting a need for prospective studies that will provide reliable estimate of HIV incidence and mortality among pregnant women, newborns, and children, they argued.
The knowledge gaps "extend to the U.S.," where a lack of FDA-approved tests and case definitions make definitive diagnosis and reporting difficult, they wrote.
On the other hand, CDC testing has shown evidence of HEV genotype 3 transmission in the U.S., including among solid-organ transplant recipients, they noted.
The agency has also supported two national labs in sharing data from HEV testing, using both antibodies and RNA. In addition, Teshale and Ward argued, epidemiologic studies are needed to define populations that have a burden of HEV and might benefit from vaccination.
In the meantime, physicians should consider HEV as part of the differential diagnosis for hepatitis, they concluded.
Xia and colleagues cautioned that a majority of cases among study participants were caused by HEV genotype 4, while the vaccine is based on genotype 1. The efficacy of the vaccine against other HEV genotypes "remains to be explored," they noted, but add that all HEV genotypes belong to the same serotype so that one vaccine can protect against any genotype.
They also noted that irregular follow-up assessments might have led to missing some HEV cases if participants did not seek medical care.
For more information about Ebola, visit Ebola Virus Disease
PATHOGEN SAFETY DATA SHEET - INFECTIOUS SUBSTANCES
CHARACTERISTICS: Ebola was discovered in 1976 and is a member of the Filoviridae family (previously part of Rhabdoviridae family, which were later given a family of their own based on their genetic structure). Five Ebola species have been identified: Zaire ebolavirus (ZEBOV), which was first identified in 1976 and is the most virulent; Sudan ebolavirus, (SEBOV); Tai Forest ebolavirus (formerly Ivory Coast ebolavirus); Ebola-Reston (REBOV), originating from the Philippines; and Bundibugyo ebolavirus (BEBOV), the most recent species discovered (2008) Footnote1Footnote3Footnote5Footnote6Footnote7.
Ebola is an elongated filamentous virus, which can vary between 800 - 1000 nm in length, and can reach up to 14000 nm long (due to concatamerization) with a uniform diameter of 80 nm Footnote2Footnote5Footnote8Footnote9. It contains a helical nucleocapsid (with a central axis), 20 - 30 nm in diameter, and is enveloped by a helical capsid, 40 - 50 nm in diameter, with 5 nm cross-striations Footnote2Footnote5Footnote8Footnote9Footnote10. The pleomorphic viral fragment may take on several distinct shapes (e.g., in the shape of a "6", a "U", or a circle), and are contained within a lipid membraneFootnote2Footnote5. Each virion contains a single-strand of non-segmented, negative-sense viral genomic RNA Footnote5Footnote11.
SECTION II - HAZARD IDENTIFICATION
PATHOGENICITY/TOXICITY: Ebola virions enter host cells through endocytosis and replication occurs in the cytoplasm. Upon infection, the virus affects the host blood coagulative and immune defence system and leads to severe immunosuppression Footnote10Footnote12. Early signs of infection are non-specific and flu-like, and may include sudden onset of fever, asthenia, diarrhea, headache, myalgia, arthralgia, vomiting, and abdominal pains Footnote13. Less common early symptoms include conjunctival injection, sore throat, rashes, and bleeding. Shock, cerebral oedema, coagulation disorders, and secondary bacterial infection may co-occur later in infection Footnote8. Haemorrhagic symptoms may begin 4 - 5 days after onset, including hemorrhagic conjunctivitis, pharyngitis, bleeding gums, oral/lip ulceration, hematemesis, melena, hematuria, epistaxis, and vaginal bleeding Footnote14. Hepatocellular damage, marrow suppression (such as thrombocytopenia and leucopenia), serum transaminase elevation, and proteinuria may also occur. Persons that are terminally ill typically present with obtundation, anuria, shock, tachypnea, normothermia to hypothermia, arthralgia, and ocular diseases Footnote15. Haemorrhagic diathesis is often accompanied by hepatic damage and renal failure, central nervous system involvement, and terminal shock with multi-organ failure Footnote1Footnote2. Contact with the virus may also result in symptoms such as severe acute viral illness, malaise, and maculopapular rash. Pregnant women will usually abort their foetuses and experience copious bleeding Footnote2Footnote16. Fatality rates range between 50 - 100%, with most dying of hypovolemic shock and multisystem organ failure Footnote17.
Pathogenicity between species of Ebola does not differ greatly in that they have all been associated with hemorrhagic fever outbreaks in humans (excluding Reston) and non-human primates. The Ebola-Zaire and Sudan strains are especially known for their virulence with up to 90% fatality rate Footnote18, with reduced virulence noted in the Tai Forest ebolavirus and the more recently discovered Bundibugyo strain, which caused a single outbreak in Uganda Footnote6Footnote7. Bundibugyo was the outbreak virus in Isiro, Democratic Republic of Congo, in 2012. Ebola-Reston was isolated from cynomolgus monkeys from the Philippines in 1989 and is less pathogenic in non-human primates. Ebola-Reston virus appears to be non-pathogenic in humans, with reported health effects limited to serological evidence of exposure as identified in 4 animal handlers working with infected non-human primates Footnote19.
EPIDEMIOLOGY: Occurs mainly in areas surrounding rain forests in equatorial Africa Footnote10with the exception of Reston, which has been documented to originate in the Philippines Footnote7. No predispositions to infection have been identified among infected persons.
The largest recorded ebolavirus outbreak to date began in March 2014, with initial cases reported in Guinea and then additional cases identified in the surrounding regions (Liberia, Sierra Leone, Nigeria). A new strain of the ZEBOV species was identified as the causative agent of the outbreak Footnote16Footnote21Footnote22.
HOST RANGE: Humans, various monkey species, chimpanzees, gorillas, baboons, and duikers are natural animal hosts for ebolavirus Footnote1Footnote2Footnote5Footnote22Footnote23Footnote24Footnote25Footnote26Footnote27Footnote28Footnote29Footnote30Footnote31. Serological evidence of immunity markers to ebolavirus in serum collected from domesticated dogs suggests asymptomatic infection is plausible, likely following exposure to infected humans or animal carrion Footnote32Footnote33. The Ebolavirus genome was discovered in two species of rodents and one species of shrew living in forest border areas, raising the possibility that these animals may be intermediary hosts Footnote34. Experimental studies of the virus have been done using mouse, pig, guinea pig, and hamster models, suggesting wild-type ebolavirus has limited pathogenicity in these models Footnote35Footnote36.
Bats are considered to be a plausible reservoir for the virus. Serological evidence of infection with ebolavirus (antibody detection to EBOV, ZEBOV, and/or REBOV) has been reported in fruit bats collected from woodland and forested areas near Ghana and Gabon, with reduced frequency of isolation from bats collected in mainland China and Bangladesh Footnote37Footnote38Footnote39Footnote40.
INFECTIOUS DOSE: Viral hemorrhagic fevers have an infectious dose of 1 - 10 organisms by aerosol in non-human primates Footnote41.
MODE OF TRANSMISSION: In an outbreak, it is hypothesized that the first patient becomes infected as a result of contact with an infected animal Footnote22. Person-to-person transmission occurs via close personal contact with an infected individual or their body fluids during the late stages of infection or after death Footnote1Footnote2Footnote22Footnote42. Nosocomial infections can occur through contact with infected body fluids for example due to the reuse of unsterilized syringes, needles, or other medical equipment contaminated with these fluids Footnote1Footnote2. Humans may be infected by handling sick or dead non-human primates and are also at risk when handling the bodies of deceased humans in preparation for funerals Footnote2Footnote10Footnote43.
In laboratory settings, non-human primates exposed to aerosolized ebolavirus from pigs have become infected, however, airborne transmission has not been demonstrated between non-human primates Footnote1Footnote10Footnote15Footnote44Footnote45. Viral shedding has been observed in nasopharyngeal secretions and rectal swabs of pigs following experimental inoculation Footnote29Footnote30.
COMMUNICABILITY: Communicable as long as blood, body fluids or organs, contain the virus. Ebolavirus has been isolated from semen 61 to 82 days after the onset of illness, and transmission through semen has occurred 7 weeks after clinical recovery Footnote1Footnote2Footnote59Footnote60.
SECTION III - DISSEMINATION
RESERVOIR: The natural reservoir of Ebola is unknown Footnote1Footnote2. Antibodies to the virus have been found in the serum of domestic guinea pigs and wild rodents, with no relation to human transmission Footnote34Footnote47. Serum antibodies and viral RNA have been identified in some bat species, suggesting bats may be a natural reservoir Footnote37Footnote38Footnote39Footnote40.
All information available on stability and viability comes from peer-reviewed literature sources depicting experimental findings and is intended to support local risk assessments in a laboratory setting.
DRUG SUSCEPTIBILITY: Unknown. Although clinical trials have been completed, no vaccine has been approved for treatment of ebolavirus. Similarly, no post-exposure measures have been reported as effective in treating ebolavirus infection in humans although several studies have been completed in animals to determine the efficacy of various treatments.
DRUG RESISTANCE: There are no known antiviral treatments available for human infections.
SUSCEPTIBILITY TO DISINFECTANTS: Ebolavirus is susceptible to 3% acetic acid, 1% glutaraldehyde, alcohol-based products, and dilutions (1:10-1:100 for ≥10 minutes) of 5.25% household bleach (sodium hypochlorite), and calcium hypochlorite (bleach powder)Footnote48Footnote49Footnote50Footnote62Footnote63. The WHO recommendations for cleaning up spills of blood or body fluids suggest flooding the area with a 1:10 dilutions of 5.25% household bleach for 10 minutes for surfaces that can tolerate stronger bleach solutions (e.g., cement, metal) Footnote62. For surfaces that may corrode or discolour, they recommend careful cleaning to remove visible stains followed by contact with a 1:100 dilution of 5.25% household bleach for more than 10 minutes.
PHYSICAL INACTIVATION: Ebola are moderately thermolabile and can be inactivated by heating for 30 minutes to 60 minutes at 60°C, boiling for 5 minutes, or gamma irradiation (1.2 x106 rads to 1.27 x106 rads) combined with 1% glutaraldehyde Footnote10Footnote48Footnote50. Ebolavirus has also been determined to be moderately sensitive to UVC radiation Footnote51.
SURVIVAL OUTSIDE HOST: Filoviruses have been reported capable to survive for weeks in blood and can also survive on contaminated surfaces, particularly at low temperatures (4°C)Footnote52Footnote61. One study could not recover any Ebolavirus from experimentally contaminated surfaces (plastic, metal or glass) at room temperature Footnote61. In another study, Ebolavirus dried onto glass, polymeric silicone rubber, or painted aluminum alloy is able to survive in the dark for several hours under ambient conditions (between 20°C and 25°C and 30–40% relative humidity) (amount of virus reduced to 37% after 15.4 hours), but is less stable than some other viral hemorrhagic fevers (Lassa) Footnote53. When dried in tissue culture media onto glass and stored at 4 °C, Zaire ebolavirus survived for over 50 days Footnote61. This information is based on experimental findings only and not based on observations in nature. This information is intended to be used to support local risk assessments in a laboratory setting.
A study on transmission of ebolavirus from fomites in an isolation ward concludes that the risk of transmission is low when recommended infection control guidelines for viral hemorrhagic fevers are followed Footnote64. Infection control protocols included decontamination of floors with 0.5% bleach daily and decontamination of visibly contaminated surfaces with 0.05% bleach as necessary.
SECTION V - FIRST AID / MEDICAL
SURVEILLANCE: Definitive diagnosis can be reached rapidly in an appropriately equipped laboratory using a multitude of approaches, including RT-PCR to detect viral RNA, ELISA based techniques to detect anti-Ebola antibodies or viral antigens, immunoelectron microscopy to detect ebolavirus particles in tissues and cells, and indirect immunofluorescence to detect antiviral antibodies Footnote1Footnote2Footnote14Footnote41. It is useful to note that the Marburg virus is morphologically indistinguishable from the ebolavirus, and laboratory surveillance of Ebola is extremely hazardous Footnote1Footnote2Footnote14Footnote54. Please see the interim biosafety guidelines for laboratories handling specimens from patients under investigationfor EVD for more information.
Note: All diagnostic methods are not necessarily available in all countries.
FIRST AID/TREATMENT: There is no effective antiviral treatment Footnote27Footnote37. Instead, treatment is supportive, and is directed at maintaining organ function and electrolyte balance and combating haemorrhage and shock Footnote22Footnote55.
PROPHYLAXIS: None. Management of the Ebola virus is solely based on isolation and barrier-nursing with symptomatic and supportive treatments Footnote8.
SECTION VI - LABORATORY HAZARDS
LABORATORY-ACQUIRED INFECTIONS: One reported near-fatal case following a minute finger prick in an English laboratory (1976) Footnote56. A Swiss zoologist contracted Ebola virus after performing an autopsy on a chimpanzee in 1994 Footnote2Footnote57. An incident occurred in Germany in 2009 when a laboratory scientist pricked herself with a needle that had just been used on a mouse infected with Ebola; however, human infection was not confirmed. Additional incidents were recorded in the US in 2004, and a fatal case in Russia in 2004 Footnote8.
SOURCES/SPECIMENS: Blood, serum, urine, respiratory and throat secretions, semen, and organs or their homogenates from human or animal hosts Footnote1Footnote2Footnote53. Human or animal hosts, including non-human primates, may represent a further source of infection Footnote54.
PRIMARY HAZARDS: Accidental parenteral inoculation, respiratory exposure to infectious aerosols/droplets, and/or direct contact with skin or mucous membranes Footnote54.
SPECIAL HAZARDS: Work with, or exposure to, infected non-human primates, rodents, or their carcasses represents a risk of human infection Footnote54.
SECTION VII - EXPOSURE CONTROLS / PERSONAL PROTECTION
RISK GROUP CLASSIFICATION: Risk Group 4 Footnote58.
PROTECTIVE CLOTHING: Personnel entering the laboratory must remove street clothing, including undergarments, and jewellery, and change into dedicated laboratory clothing and shoes, or don full coverage protective clothing (i.e., completely covering all street clothing). Additional protection may be worn over laboratory clothing when infectious materials are directly handled, such as solid-front gowns with tight fitting wrists, gloves, and respiratory protection. Eye protection must be used where there is a known or potential risk of exposure to splashes.
OTHER PRECAUTIONS: All activities with infectious material should be conducted in a biological safety cabinet (BSC) in combination with a positive pressure suit, or within a class III BSC line. Centrifugation of infected materials must be carried out in closed containers placed in sealed safety cups, or in rotors that are unloaded in a biological safety cabinet. The integrity of positive pressure suits must be routinely checked for leaks. The use of needles, syringes, and other sharp objects should be strictly limited. Open wounds, cuts, scratches, and grazes should be covered with waterproof dressings. Additional precautions should be considered with work involving animal activities.
SECTION VIII - HANDLING AND STORAGE
SPILLS: Allow aerosols to settle and, wearing protective clothing, gently cover spill with paper towels and apply suitable disinfectant, starting at the perimeter and working towards the centre. Allow sufficient contact time before clean-up.
DISPOSAL: Decontaminate all materials for disposal from the containment laboratory by steam sterilisation, chemical disinfection, incineration or by gaseous methods. Contaminated materials include both liquid and solid wastes.
STORAGE: In sealed, leak-proof containers that are appropriately labelled and locked in a Containment Level 4 laboratory.
SECTION IX - REGULATORY AND OTHER INFORMATION
REGULATORY INFORMATION: The import, transport, and use of pathogens in Canada is regulated under many regulatory bodies, including the Public Health Agency of Canada, Health Canada, Canadian Food Inspection Agency, Environment Canada, and Transport Canada. Users are responsible for ensuring they are compliant with all relevant acts, regulations, guidelines, and standards.
UPDATED: August 2014.
PREPARED BY: Centre for Biosecurity, Public Health Agency of Canada.
Although the information, opinions and recommendations contained in this Pathogen Safety Data Sheet are compiled from sources believed to be reliable, we accept no responsibility for the accuracy, sufficiency, or reliability or for any loss or injury resulting from the use of the information. Newly discovered hazards are frequent and this information may not be completely up to date.
Plague. (2004). In R. G. Darling, & J. B. Woods (Eds.), USAMRIID's Medical Management of Biological Casualties Handbook (5th ed., pp. 40-44). Fort Detrick M.D.: USAMRIID.
Footnote2
Acha, P. N., & Szyfres, B. (2003). In Pan American Health Organization (Ed.), Zoonoses and Communicable Diseases Common to Man and Animals (3rd ed., pp. 142-145). Washington D.C.: Pan American Health Organization.
Footnote3
International Committee on Taxonomy of Viruses (2013 Release). Virus Taxonomy. Ebolavirus. http://www.ictvonline.org/virusTaxonomy.asp
Footnote4
Kuhn, J. H., Becker, S., Ebihara, H., Geisbert, T. W., Johnson, K. M., Kawaoka, Y., Lipkin IW, Negredo AI, Netesov SV, Nichol ST, Palacios G, Peters CJ, Tenorio A, Volchokov VE, & Jahrling, P. B. (2010). Proposal for a revised taxonomy of the family Filoviridae: classification, names of taxa and viruses, and virus abbreviations. Archives of virology, 155(12), 2083-2103.
Footnote5
Sanchez, A. (2001). Filoviridae: Marburg and Ebola Viruses. In D. M. Knipe, & P. M. Howley (Eds.), Fields virology (4th ed., pp. 1279-1304). Philadelphia, PA.: Lippencott-Ravenpp.
Footnote6
Takada, A., & Kawaoka, Y. (2001). The pathogenesis of Ebola hemorrhagic fever. Trends in Microbiology, 9(10), 506-511.
Footnote7
Towner, J. S., Sealy, T. K., Khristova, M. L., Albarino, C. G., Conlan, S., Reeder, S. A., Quan, P. L., Lipkin, W. I., Downing, R., Tappero, J. W., Okware, S., Lutwama, J., Bakamutumaho, B., Kayiwa, J., Comer, J. A., Rollin, P. E., Ksiazek, T. G., & Nichol, S. T. (2008). Newly discovered ebola virus associated with hemorrhagic fever outbreak in Uganda. PLoS Pathogens, 4(11), e1000212.
Footnote8
Feldmann, H. (2010). Are we any closer to combating Ebola infections? Lancet, 375(9729), 1850-1852. doi:10.1016/S0140-6736(10)60597-1.
Footnote9
Beran, G. W. (Ed.). (1994). Handbook of Zoonosis, Section B: Viral (2nd ed.). Boca Raton, Florida: CRC Press, LLC.
Footnote10
Mwanatambwe, M., Yamada, N., Arai, S., Shimizu-Suganuma, M., Shichinohe, K., & Asano, G. (2001). Ebola hemorrhagic fever (EHF): mechanism of transmission and pathogenicity. Journal of Nippon Medical School.68(5), 370-375.
Footnote11
Sanchez, A., Kiley, M. P., Klenk, H. D., & Feldmann, H. (1992). Sequence analysis of the Marburg virus nucleoprotein gene: comparison to Ebola virus and other non-segmented negative-strand RNA viruses. The Journal of General Virology, 73 (Pt 2)(Pt 2), 347-357.
Footnote12
Harcourt, B. H., Sanchez, A., & Offermann, M. K. (1999). Ebola virus selectively inhibits responses to interferons, but not to interleukin-1beta, in endothelial cells. Journal of Virology, 73(4), 3491-3496.
Footnote13
Bwaka, M. A., Bonnet, M. J., Calain, P., Colebunders, R., De Roo, A., Guimard, Y., Katwiki, K. R., Kibadi, K., Kipasa, M. A., Kuvula, K. J., Mapanda, B. B., Massamba, M., Mupapa, K. D., Muyembe-Tamfum, J. J., Ndaberey, E., Peters, C. J., Rollin, P. E., Van den Enden, E., & Van den Enden, E. (1999). Ebola hemorrhagic fever in Kikwit, Democratic Republic of the Congo: clinical observations in 103 patients. The Journal of Infectious Diseases, 179 Suppl 1, S1-7.
Footnote14
Zilinskas, R. A. (Ed.). (2000). Biololgical Warfare - Modern Offense and Defense. Boulder, Colorado, USA: Lynne Rienner Publishers, Inc.
Footnote15
Feigin, R. D. (Ed.). (2004). Textbook of Pediatric Infectious Diseases (5th ed.). Philadelphia, USA: Elsevier, Inc.
Footnote16
Baize, S., Pannetier, D., Oestereich, L., Rieger, T., Koivogui, L., Magassouba, N., Soropogui, B., Sow, M. S., Keita, S., De Clerck, H., Tiffany, A., Dominguez, G., Loua, M., Traore, A., Kolie, M., Malano, E. R., Heleze, E., Bocquin, A., Mely, S., Raoul, H., Caro, V., Cadar, D., Gabriel, M., Pahlmann, M., Tappe, D., Schmidt-Chanasit, J., Impouma, B., Diallo, A.K., Formenty, P., Van Herp, M., & Gunther, S. (2014). Emergence of Zaire Ebola Virus Disease in Guinea - Preliminary Report. The New England Journal of Medicine. Epub ahead of print.
Footnote17
Casillas, A. M., Nyamathi, A. M., Sosa, A., Wilder, C. L., & Sands, H. (2003). A current review of Ebola virus: pathogenesis, clinical presentation, and diagnostic assessment. Biological Research for Nursing, 4(4), 268-275.
Footnote18
World Health Organization. Ebola Virus Disease - Fact Sheet N°103. Updated April 2014.
Footnote19
Centers for Disease Control and Prevention. (1990). Epidemiologic notes and reports updates: filovirus infection in animal handlers. MMWR, 39, 221.
Footnote20
World Health Organization. Global Alert and Response (GAR) - Ebola virus disease update - West Africa. Disease outbreak news. August 6 2014
Footnote21
Centres for Disease Control. 2014 Ebola Outbreak in West Africa (Guinea, Liberia, Sierra Leone and Nigeria. August 6 2014
Footnote22
Bausch, D. G., Jeffs B.S.A.G, & Boumandouki, P. (2008). Treatment of Marburg and Ebola haemorrhagic fevers: a strategy for testing new drugs and vaccines under outbreak conditions. Antiviral Res., 78(1), 150-161.
Footnote23
WHO Disease Outbreak News - Ebola Haemorrhagic Fever in the Democratic Republic of Congo. (2007). 2008
Footnote24
WHO Disease Outbreak News - Ebola Haemorrhagic Fever in Uganda - Update. (2007). 2008
Footnote25
Formenty, P., Boesch, C., Wyers, M., Steiner, C., Donati, F., Dind, F., Walker, F., & Le Guenno, B. (1999). Ebola virus outbreak among wild chimpanzees living in a rain forest of Cote d'Ivoire. The Journal of Infectious Diseases, 179 Suppl 1, S120-6. doi:10.1086/514296.
Footnote26
Bray, M. (2003). Defense against filoviruses used as biological weapons. Antiviral Research, 57(1-2), 53-60.
Footnote27
Leroy, E. M., Rouquet, P., Formenty, P., Souquière, S., Kilbourne, A., Froment, J., Bermejo, M., Smit, S., Karesh, W., Swanepoel, R., Zaki, S. R., & Rollin, P. E. (2004). Multiple Ebola Virus Transmission Events and Rapid Decline of Central African Wildlife. Science, 303(5656), 387-390.
Footnote28
Nfon, C. K., Leung, A., Smith, G., Embury-Hyatt, C., Kobinger, G., & Weingartl, H. M. (2013). Immunopathogenesis of severe acute respiratory disease in Zaire ebolavirus-infected pigs. PloS one, 8(4), e61904.
Footnote29
Kobinger, G. P., Leung, A., Neufeld, J., Richardson, J. S., Falzarano, D., Smith, G., Tierney, K., Patel, A., & Weingartl, H. M. (2011). Replication, pathogenicity, shedding, and transmission of Zaire ebolavirus in pigs. Journal of Infectious Diseases, jir077.
Footnote30
Marsh, G. A., Haining, J., Robinson, R., Foord, A., Yamada, M., Barr, J. A., Payne, J., White, J., Yu, M., Bingham, J., Rollin, P. E., Nichol, S. T., Wang, L-F., & Middleton, D. (2011). Ebola Reston virus infection of pigs: clinical significance and transmission potential. Journal of Infectious Diseases, 204(suppl 3), S804-S809.
Footnote31
Morris, K. (2009). First pig-to-human transmission of Ebola Reston virus.9(3), 148.
Footnote32
Allela, L., Bourry, O., Pouillot, R., Délicat, A., Yaba, P., Kumulungui, B., Rougquet, P., Gonzalez, J-P., & Leroy, E. M. (2005). Ebola virus antibody prevalence in dogs and human risk. Emerg Infect Dis, 11(3), 385-90.
Footnote33
Olson, S. H., Reed, P., Cameron, K. N., Ssebide, B. J., Johnson, C. K., Morse, S. S., Karesh, W. B.., Mazet, J. A. K., & Joly, D. O. (2012). Dead or alive: animal sampling during Ebola hemorrhagic fever outbreaks in humans. Emerging health threats journal, 5.
Footnote34
Morvan, J. M., Nakouné, E., Deubel, V., & Colyn, M. (2000). Ebola virus and forest ecosystem. [Écosystèmes forestiers et virus Ebola] Bulletin De La Societe De Pathologie Exotique, 93(3), 172-175.
Footnote35
Connolly, B. M., Steele, K. E., Davis, K. J., Geisbert, T. W., Kell, W. M., Jaax, N. K., & Jahrling, P. B. (1999). Pathogenesis of experimental Ebola virus infection in guinea pigs. The Journal of Infectious Diseases, 179 Suppl 1, S203-17.
Footnote36
Ebihara, H., Zivcec, M., Gardner, D., Falzarano, D., LaCasse, R., Rosenke, R., Long, D., Haddock, E., Fischer, E., Kawaoka, Y., & Feldmann, H. (2012). A Syrian golden hamster model recapitulating Ebola hemorrhagic fever. Journal of Infectious Diseases, jis626.
Footnote37
Leroy, E. M., Kumulungui, B., Pourrut, X., Rouquet, P., Hassanin, A., Yaba, P., Délicat, A., Paweska, J. T., Gonzalez, J., & Swanepoel, R. (2005). Fruit bats as reservoirs of Ebola virus. Nature, 438(7068), 575-576.
Footnote38
Hayman, D. T., Yu, M., Crameri, G., Wang, L. F., Suu-Ire, R., Wood, J. L., & Cunningham, A. A. (2012). Ebola virus antibodies in fruit bats, Ghana, West Africa. Emerging infectious diseases, 18(7), 1207.
Footnote39
Yuan, J., Zhang, Y., Li, J., Zhang, Y., Wang, L. F., & Shi, Z. (2012). Serological evidence of ebolavirus infection in bats, China. Virol. J, 9, 236.
Footnote40
Olival, K. J., Islam, A., Yu, M., Anthony, S. J., Epstein, J. H., Khan, S. A., Khan, S. U., Crameri, G., Wang, L-F., Lipkin, W. I., Luby, S. P., & Daszak, P. (2013). Ebola virus antibodies in fruit bats, Bangladesh. Emerging infectious diseases, 19(2), 270.
Footnote41
Franz, D. R., Jahrling, P. B., Friedlander, A. M., McClain, D. J., Hoover, D. L., Bryne, W. R., Pavlin, J. A., Christopher, G. W., & Eitzen, E. M. (1997). Clinical recognition and management of patients exposed to biological warfare agents. Jama, 278(5), 399-411.
Footnote42
Arthur, R. R. (2002). Ebola in Africa--discoveries in the past decade. Euro Surveillance : Bulletin Europeen Sur Les Maladies Transmissibles = European Communicable Disease Bulletin, 7(3), 33-36.
Footnote43
Hewlett, B. S., & Amolat, R. P. (2003). Cultural contexts of Ebola in Northern Uganda. Emerging Infectious Diseases, 9(10), 1242-1248.
Footnote44
Reed, D. S., Lackemeyer, M. G., Garza, N. L., Sullivan, L. J., & Nichols, D. K. (2011). Aerosol exposure to Zaire ebolavirus in three nonhuman primate species: differences in disease course and clinical pathology. Microbes and Infection, 13(11), 930-936.
Footnote45
Twenhafel, N. A., Mattix, M. E., Johnson, J. C., Robinson, C. G., Pratt, W. D., Cashman, K. A., Wahl-Jensen, V., Terry, C., Olinger, G. G., Hensley, L. E., & Honko, A. N. (2012). Pathology of experimental aerosol Zaire ebolavirus infection in rhesus macaques. Veterinary Pathology Online, 0300985812469636.
Footnote46
Weingartl, H. M., Embury-Hyatt, C., Nfon, C., Leung, A., Smith, G., & Kobinger, G. (2012). Transmission of Ebola virus from pigs to non-human primates. Scientific reports, 2.
Footnote47
Stansfield, S. K., Scribner, C. L., Kaminski, R. M., Cairns, T., McCormick, J. B., & Johnson, K. M. (1982). Antibody to Ebola virus in guinea pigs: Tandala, Zaire. The Journal of Infectious Diseases, 146(4), 483-486.
Footnote48
Mitchell, S. W., & McCormick, J. B. (1984). Physicochemical inactivation of Lassa, Ebola, and Marburg viruses and effect on clinical laboratory analyses. Journal of Clinical Microbiology, 20(3), 486-489.
Footnote49
Elliott, L. H., McCormick, J. B., & Johnson, K. M. (1982). Inactivation of Lassa, Marburg, and Ebola viruses by gamma irradiation. Journal of Clinical Microbiology, 16(4), 704-708.
Footnote50
World Health Organization. Interim Infection Control Recommendationsfor Care of Patients with Suspected or Confirmed Filovirus (Ebola, Marburg) Haemorrhagic Fever. March 2008
Footnote51
Sagripanti, J. L., & Lytle, C. D. (2011). Sensitivity to ultraviolet radiation of Lassa, vaccinia, and Ebola viruses dried on surfaces. Archives of virology, 156(3), 489-494.
Footnote52
Belanov, E. F., Muntianov, V. P., Kriuk, V., Sokolov, A. V., Bormotov, N. I., P'iankov, O. V., & Sergeev, A. N. (1995). [Survival of Marburg virus infectivity on contaminated surfaces and in aerosols]. Voprosy virusologii, 41(1), 32-34.
Footnote53
Sagripanti, J-L., Rom, A.M., Holland, L.E. (2010) Persistence in darkness of virulent alphaviruses, Ebola virus, and Lass virus deposited on solid surfaces. Arch Virol. 155: 2035-9.
Footnote54
Biosafety in Microbiological and Biomedical Laboratories (BMBL) (2007). In Richmond J. Y., McKinney R. W. (Eds.), . Washington, D.C.: Centers for Disease Control and Prevention.
Footnote55
Clark, D. V., Jahrling, P. B., & Lawler, J. V. (2012). Clinical Management of Filovirus-Infected Patients. Viruses, 4(9), 1668-1686.
Footnote56
Emond, R. T. D., Evans, B., Bowen, E. T. W., & Lloyd, G. (1977). A case of Ebola virus infection. British Medical Journal, 2(6086), 541-544.
Footnote57
Formenty, P., Hatz, C., Le Guenno, B., Stoll, A., Rogenmoser, P., & Widmer, A. (1999). Human infection due to Ebola virus, subtype Cote d'Ivoire: Clinical and biologic presentation. Journal of Infectious Diseases, 179(SUPPL. 1), S48-S53.
Footnote58
Human pathogens and toxins act. S.C. 2009, c. 24, Second Session, Fortieth Parliament, 57-58 Elizabeth II, 2009. (2009).
Footnote59
Rowe AK, Bertolli J,Khan AS,et al. Clinical, virologic, and immunologic follow-up of convalescent Ebola hemorrhagic fever patients and their household contacts, Kikwit, Democratic Republic of the Congo. Commission de Lutte contre les Epidemies à Kikwit. J Infect Dis 1999;179 (Suppl 1):S28-35.
Footnote60
Rodriguez LL, De Roo A, Guimard Y, et al. Persistence and genetic stability of Ebola virus during the outbreak in Kikwit, Democratic Republic of the Congo, 1995. J Infect Dis 1999;179 (Suppl 1):S170-6.
Footnote61
Piercy, T.J., Smither, S.J., Steward, J.A., Eastaugh, L., Lever, M.S. (2010) The survival of filoviruses in liquids, on solid substrates and in a dynamic aerosol. J Appl Microbiol. 109(5): 1531-9.
Footnote62
World Health Organization (2010). WHO best practices for injections and related procedures toolkit. March 2010. http://whqlibdoc.who.int/publications/2010/9789241599252_eng.pdf?ua=1
Footnote63
World Health Organization (2014). Interim infection prevention and control guidance for care of patients with suspected or confirmed filovirus haemorrhagic fever in health-care settings, with focus on Ebola. August 2014. http://www.who.int/csr/resources/who-ipc-guidance-ebolafinal-09082014.pdf
Footnote64
Baush, D.G., Towner, J.S., Dowell, S.F., Kaducu, F., Lukwiya, M., Sanchez, A., Nichol, S.T., Ksiazek, T.G., Rollin, P.E. (2007) Assessment of the Risk of Ebola virus Transmission from Bodily Fluids and Fomites. JID. 196 (Suppl 2).
Current 2014 Ebolla Outbreak explained: Click here for videoREAD about the history of Ebolla in the best seller The HOT ZONE - this video explains how HIV & other "bushmeat" transmitted diseases" move as a Zoonosis from other species (carriers) to man CLICK HERE for TED talk on the Global Virus Initiative.
It was first used on an experimental basis to treat some people with Ebola virus disease during the 2014 West African Ebola outbreak, but as of August 2014 it had not yet been tested in a clinical trial to support widespread usage in humans; its safety and efficacy are not known.[3][4]
ZMapp is composed of three monoclonal antibodies (mAbs) that have been humanized by genetic engineering.[7] The components are humanized monoclonal antibody c13C6 from a previously-existing antibody cocktail called "MB-003" and two humanized mAbs from a different antibody cocktail called ZMab, c2G4 and c4G7.[2]
Researchers looking at slides of cultures of cells that make monoclonal antibodies. These are grown in a lab and the researchers are analyzing the products to select the most promising antibodies.
ZMab was created by Defyrus, a Toronto-based biodefense company, based on years of funding from the Public Health Agency of Canada.[13] The identification of the optimal components from MB-003 and ZMab was carried out at the Public Health Agency of Canada’s National Microbiology Laboratory in Winnipeg.[14]
Leaf Bio licensed the pre-existing cocktails from each of Mapp and Defyrus and collaborated with them to create ZMapp, which Leaf will commercialize.[9] Mapp remains involved in the production of the drug, through its contracts with Kentucky BioProcessing, a subsidiary of Reynolds American.[1]
MB-003 is a cocktail of three human or human–mouse chimaeric mAbs: c13C6, h13F6 and c6D8.[2] A study published in September 2012 found that rhesus macaques infected with Ebola virus (EBOV) survived when receiving MB-003 (mixture of 3 chimeric monoclonal antibodies) one hour after infection. When treated 24 or 48 hours after infection, four of six animals survived and had little to no viremia and few, if any, clinical symptoms.[15]
ZMAb is a cocktail of three mouse mAbs: m1H3, m2G4 and m4G7.[2] A study published in November 2013 found that EBOV-infected macaque monkeys survived after being given a therapy with a combination of three EBOV surface glycoprotein (EBOV-GP)-specific monoclonal antibodies (ZMAb) within 24 hours of infection. The authors concluded that post-exposure treatment and a second lethal exposure after 10 and 13 weeks resulted in a robust immune response.[16]
A 2014 paper described how Mapp and its collaborators at Public Health Agency of Canada, Kentucky BioProcessing, and the National Institute of Allergy and Infectious Diseases first humanized the three antibodies comprising ZMAb, then tested combinations of MB-003 and the humanized ZMAb antibodies in guinea pigs and then primates to determine the best combination, which turned out to be c13C6 from MB-003 and two humanized mAbs from ZMAb, c2G4 and c4G7. This is ZMapp.[2]
In an experiment also published in the 2014 paper, 21 rhesus macaque primates were infected with the Kikwit Congolese variant of EBOV. Three primates in the control arm were given a non-functional antibody, and the 18 in the treatment arm were divided into three groups of six. All primates in the treatment arm received three doses of ZMapp, spaced 3 days apart. The first treatment group received its first dose on 3rd day after being infected; the second group on the 4th day after being infected, and the third group, on the 5th day after being infected. All three primates in the control group died; all 18 primates in the treatment arm survived.[2] Mapp then went on to show that ZMapp inhibits replication of a Guinean strain of EBOV in cell cultures.[17]
To create a system to produce the humanized mAbs at commercial scale, Mapp used a process called "Rapid Antibody Manufacturing Platform" (RAMP), using magnICON (ICON Genetics) viral vectors. In a rapid and scalable process called "magnifection,"[18] tobacco plants are infected with the viruses, usingAgrobacterium cultures.[1][15][19] Subsequently, antibodies are extracted and purified from the plants. Once the genes encoding the humanized mAbs are in hand, the entire tobacco production cycle is believed to take a few months.[20]
In the US, the FDA's Animal Efficacy Rule can be used, often in combination with a Phase I clinical trial, to demonstrate reasonable safety for a drug, to obtain permission to treat urgently sick people with the drug under the FDA's Expanded access program. The Animal Efficacy Rule exists because the normal path for testing the safety and efficacy of drugs is not possible for diseases caused by dangerous pathogens or toxins.[20][21] The FDA has allowed two drugs, ZMapp and an RNA interference drug called "TKM-Ebola", to be used in Americans suffering from Ebola virus disease under these programs.[22] Other countries have similar programs to allow early access through named patient programs.
In 2014, Samaritan's Purse worked with the FDA and Mapp Biopharmaceutical to make the drug available to two of its health workers who were infected by Ebola virus during their work in Liberia, under the Expanded access program.[20] At the time, there were only a few doses of ZMapp in existence.[20] Both workers received the drug and were transported to the US, where they recovered and were then released from the hospital.[23][24][25] A 75-year-old Spanish priest who was infected with Ebola virus in Liberia received ZMapp in cooperation with Spanish health authorities, and died shortly thereafter.[26][27]
The west African nation of Liberia secured enough ZMapp to treat three Liberians with the disease, one of whom died.[28][29]
A British nurse who contracted Ebola virus disease while working in Sierra Leone, was transported to the UK and treated with ZMapp, and recovered.[30][31] All of the cases mentioned above occured in August 2014.
Mapp announced on August 11, 2014 that its supplies of ZMapp had been exhausted.[32]
The lack of drugs and unavailability of experimental treatment in the most affected regions of the West African Ebola virus outbreak spurred some controversy.[20]
On August 6, 2014, Peter Piot, who co-discovered Ebola virus, and other scientists, including the director of the Wellcome Trust, called for the release of ZMapp for affected African nations.[33] The fact that the drug was first given to Americans and a European and not to Africans, according to the Los Angeles Times, "provoked outrage, feeding into African perceptions of Western insensitivity and arrogance, with a deep sense of mistrust and betrayal still lingering over the exploitation and abuses of the colonial era."[33]
However, in light of the history of exploitation and abuses, Dr. Salim S. Abdool Karim (director of an AIDS research center in South Africa), responding to a question on how people may have reacted if ZMapp and other drugs would have been used first in Africans, said, “It would have been the front-page screaming headline: 'Africans used as guinea pigs for American drug company’s medicine.'"[20]
Regarding whether ZMapp should be fast-tracked for approval or be made available to sick patients outside of the United States, U.S. President Barack Obamastated on August 6, 2014, “I think we have to let the science guide us."[34]
An international team of researchers has traced the "epidemic ignition" of HIV/AIDS to 1920s Kinshasa, what is now the capital city of the Democratic Republic of the Congo.
Research findings published in the latest issue of Science trace the origins of the outbreak to Kinshasa in the 1920s, where epidemiologists believe it emerged from a "perfect storm" of explosive population growth, a booming sex industry, burgeoning public transportation networks, and the use of unsterilized needles in health clinics. Here's The Guardian's Ian Sample:
An international team of scientists led by the universities of Oxford in Britain and Leuven in Belgium reconstructed the history of the HIV pandemic using historical records and DNA samples of the virus dating back to the late 1950s. The DNA allowed them to draw up a family tree of the virus that traced its ancestry through time and space. Using statistical models they could push farther back than the 1950s and locate the origin of the pandemic in 1920s Kinshasa.
People with HIV in central Africa at the time did not have specific symptoms that would have been written down in their medical records. The virus causes the immune system to collapse, leaving people open to all manner of infections. "For an epidemic like HIV where we're trying to track back to before it was even discovered, genetics is the only source of information we have," said Oliver Pybus, an evolutionary biologist at Oxford University and senior author on the study.
The genetic data suggests that pandemic HIV spread rapidly through the Democratic Republic of the Congo, a country the size of western Europe. From the late 1930s to the early 1950s, the virus spread by rail and river to Mbuji-Mayi and Lubumbashi in the south and Kisangani in the north. There the virus took hold and formed secondary reservoirs from where it spread to countries in southern and eastern Africa.
To be clear: The AIDS virus is believed to have spilled over into the human population years before it gained purchase in Kinshasa, but conditions there were such that the infection was first able to proliferate and spread. It did so quietly at first, stealing its steady way through the surrounding area for several decades before thundering, deadly and swift, across the globe.
Whooping cough—which killed just six Americans in 1995—is back big-time, especially on the Westside of Los Angeles, thanks to stupid and stubborn rich people who refuse to vaccinate on the schedule recommended by the Centers for Disease Control. (LA has the most whooping cough cases of any California county this year: 1,317.) The Hollywood Reporter has waded into the apparently-conscience-free world of the Westside anti-vaxxers and found a legion of selfish parents enabled by fancy doctors and often expensive schools, which obviously have to balance potential lost tuition from angry parents with potential lost tuition from kids who die of measles.
When parents want to enroll their students in school without proper vaccinations, they have to file a personal belief exemption form and THR also crunched the numbers on those, revealing that "wealthy Westside kids — particularly those attending exclusive, entertainment-industry-favored child care centers, preschools and kindergartens — are far more likely" to be un-vaxxed and the rates could soon reach a public health tipping-point.
Here's how bad it is: "The region stretching from Malibu south to Marina del Rey and inland as far as La Cienega Boulevard (and including Santa Monica, Pacific Palisades, Brentwood, West Hollywood and Beverly Hills) averaged a 9.1 percent PBE level among preschoolers for the 2013-14 school year — a 26 percent jump from two years earlier." LA County as a whole had just a 2.2 percent level during the same period. Many individual schools have much higher numbers—as high as 88 percent—that put them about on par with "developing countries like Chad and South Sudan."
There is no proven link between vaccination and any serious medical problem (the whole autism thing was debunked years ago), but some parents—found inseveralanalyses to be the rich and well-educated ones—think they know better and, furthermore, that keeping their children from possibly developing eczema or whatever is more important than maintaining hard-earned herd immunity in their communities (when a certain percentage of the population is vaccinated, everyone is protected; so far there have been few enough un-vaxxed children that they can piggyback on that herd immunity).
The health effect on Los Angeles is real: one pediatrician says "We have seen ahuge pertussis outbreak in Malibu and the Palisades area." But Westside parents do not care about all those other sick kids; as "the most influential pediatrician among Westside vaccine decliners" says: "[Herd immunity] enters every single discussion I have with parents … But it isn't the predominant topic because they don't come in with a 2-month-old baby and go, 'What's the best thing for Los Angeles?' "
California's dark legacy of Eugenic forced sterilizations
By Elizabeth Cohen and John Bonifield, CNN
Sterilization victims seek compensation
(CNN) - Six decades ago, Charlie Follett was a teenager living in California's Sonoma State Home. As he did most days, Follett sat in a field, singing popular songs to himself, enjoying the sunshine and the solitude. Suddenly, someone came outside to get Follett and brought him to the hospital. They told him to lie down on an operating table, and then the needle came out. "First, they shot me with some kind of medicine. It was supposed to deaden the nerves," he said. "Then the next thing I heard was snip, snip, and that was it." The doctors didn't tell Follett what they were doing, but he knew anyway. Other boys at the Sonoma State Home had told him how much it hurt to have a vasectomy. Now it was his turn. "When they did (my right side), it seemed like they were pulling my whole insides out," said Follett, now 82 and living in Stockton. California: Leader in forced sterilizations Follett was one of 20,000 Californians forcibly sterilized by the state from 1909 to 1963. The goal was to rid society of people thought to be undesirable: people labeled "feeble-minded" or "defectives." "It's one of the most horrific and shameful chapters in California's history," said Los Angeles civil rights attorney Areva Martin. Thirty-two states had eugenics programs, but California was in a league of its own.
CNN's Lindsey Bomnin contributed to this story.
NOTE: The most common correlations with an "A" in Microbiology are: PERFECT CLASS ATTENDANCE, forming & meeting a regular weekly "study" group, and a previous "A" grade in an advanced Science class OPORTUNITIES IN NURSING- get experienced NOW before you apply - click on the clinical internship notice link in yellow/blue below!
NO FOOD or drink cups can be visible during lab/Chairs UNDER the table/inside something - please!
The Course Calendar (menu right) will show you approximate dates for major EXAMS, Tests, and Microbiology 40 meetings... please see the Daily Agenda for confirmation each week or see this DAILY ANNOUNCEMENT PAGE - do not contact the admin or Chair if you are confused - EMAIL or GOOGLE+ ME!
NOTE: This site utilizes Google Drive, a file storage and sharing cloud service. It is not required to have a Google or Google Drive account. Links for access to course material posted to Google Drive can be found on this site.
All course material posted to this site, including the site itself, can be accessed on all desktop browsers including Explorer, Chrome, Firefox, Safari and Opera; as while as their mobile browser counterparts in addition to Skyfire, S60, Dolphin, UC and Blackberry browsers. Please contact Professor Hicks immediately for any problems encountered on your device or browser.
CONTACT INFORMATION
Professor Donald R Hicks
hicksmicro@gmail.com (DO NOT CALL or LEAVE A MESSAGE!)
Terence & Nancy - LACC Micro Labtech Assistant;
(323) 953-4000 ext 2802 or see them in SC-110 Naira - GCC Micro Labtech (818) 240-1000 x 5361
OFFICE HOURS: MyOffice hours are 30 min to 1 hour before and 30 min to1 hour after each class, all during the Microbiology 40 lab at LACC in SC-112 (FRIDAYS from 4th to 14th week each term) or by appointment in Science Building (SCI) 110/112. My office is located on the 2nd floor in SCI #218-S (enrolled students may take the elevator to the 2nd, exit right and proceed through the first door to the right). ALLAppointments should be made and confirmed by email.
Please note that the college voice-messages system in my office are checked only weekly. Emails will be answered immediately. You may also ask questions that apply and are seen by everyone in the class using google+ (hicksmicro@gmail.com) use my voice mail at home or text ONLY IN EMERGENCY!
THE LACC Sheriff's Office EMERGENCY TELEPHONE NUMBER is: 323-662-5276 or from a campus phone press #3; call the LA CITY COLLEGE Sheriff's Office BEFORE 911! THE GCC College Police EMERGENCY TELEPHONE NUMBER is: 818-409-5911 or 4000 from any GCC College phone; call the GCC College Police FIRST in emergencies before calling 911 as they respond immediately!
EMAIL RULES
The college supplies each student with a personal private unique email address which must be used in all communication. Students who do not receive emails from Professor Hicks during the first or subsequent weeks must check with enrollment personnel in the administration building immediately to verify their correct email address has been provided to the instructor and that they understand how to access and utilize this official email communication service provided by the college. BECAUSE I RECEIVE HUNDREDS OF EMAILS A DAY AND THUS YOUR IMPORTANT COMMUNICATION TO ME MIGHT GET "LOST," DO NOT USE THE PROFESSOR'S OFFICIAL LACC EMAIL ADDRESS FOR CLASS QUESTIONS use:hicksmicro@gmail.com
All emails must include in the SUBJECT LINE:your Last name, first name, your course and class number, your student ID# followed by a brief topic statement (for example in the subject line put something like this: Hicks, Donald ID#34456555 M1 #3432; Absent illness 7/1/13)
All information wished to be communicated must be written in the body of your email. Also within the body of your email, state whether an attachment is included with your email. Only "Word" documents will be accepted as attachments. This includes (.doc) and (.docx) file formats.
Do not email questions on test days or the night before any evaluation. They will not be answered as I am preparing the paperwork for the evaluation and lack time to properly answer late questions.
COURSE CALENDAR This is a LEVEL 3 (trust level) Guide to the Course Dates, the LEVEL 2 is the Daily Agenda and the BEST or LEVEL 1 is "The Week in Brief" found on the INDEX page of the Microblogsite...
WEEK # of Fall 2014
LECTURE TOPIC/CHAPTER
LABORATORY TOPIC
EVALUATION
Week 1 & 2
Week 1 has 1 class day and a HOLIDAY SEPTEMBER 1 Monday is a HOLIDAY- no classes
Weeks of 8/24 & 8/31 NO M40
Class Intro/Syllabus “What is Science/Scientific Method” from the INTRO NOTES; OYO: Intro to Textbook, Chapter 1 Science and Why Study Microbiology plus Chapter 2 Chemistry review
Check lab supply fee receipt; Aseptic Technique/Universal Precautions/SAFETY Page including DISCARDS and signature to SAFETY PAGE returned to instructor
Keeping the Lab Record Book
Seat/Scope/Lab Partner assignments
Pop Quiz Syllabus/Safety
Week 3
Week of 9/7 NO M40
“What is Science” Intro Notes continued
Making your Lab Manual Cards lecture and demos Assign seats/lab drawers/partners check out scopes... discuss Scope Focusing and lab videos
Chapter Test #1: Essay 1 “What is Science” 2 page essay and short answers
Week 4
Week of 9/14 NO M40
Chapter 3
“The Microscope”
How to Focus, Store, & Clean the Microscope
How to Properly Wash a Slide
Preparation of a Smear
The Simple Stain
The Negative or Capsular Stain LABS: WE ARE DOING the Scope focusing lab (RBCells) & Cheek Negative Stain/Capsular Stain in class 1st class lab - focus RBC+cheek negative stain 2nd class lab - We are doing Smear from Agar and Simple & Gram Stains 2nd class lab
Pop Quiz: Chapter 3 Scope Care, Use and Storage
Week 5
Week of 9/21 1st M40 Friday 9-10 AM REGISTRATION and Discussion of Requirements Instructor HELP - Practicing Smears Gram and AF Staining from 10-12 ONLY
Ch 3/Simple vs Differential Staining
The Gram Stain Lecture + Chapter 4 Cells (CW/PM structures); Acid Fast and Endospore Stain lecture
Simple vs Differential Staining; Smear Prep from Agar and Broth
1st class labis the 1st Gram Stain practice 2nd class lab is the 1st Acid Fast Staining practice perhaps some Endospore Staining
Chapter Test #2: 100 multiple choice + 2 essays over Ch 3 + Safety, Smears, Stains, the Microscope care, focusing, cleaning, & storage
Week 6
Week of 9/28 2nd M40 Practice ALL STAINS for LP1 FRIDAY 9-12
Ch 3/The Acid Fast Stain Lecture
The Endospore Stain practicebegins Smear Prep from Agar and Broth; Gram, Acid Fast Staining & Endospore Staining practice
1st class labis the 1st Endospore Stain practice
2nd class lab is all 3 stains practice
Pop Quiz Unknown Cards
Week 7
Week of 10/5 3rd M40 Practice and LAST LP1 PRACTICE ALL STAINS for LP1 FRIDAY 9-12 & Saturday 7-9 PM
Ch 3 + Chapter 9 Taxonomy & Lecture Review for LP1 and Lab Practice Endospore Stain
Practice Scope focusing and care; Smears; 3 Differential Stains for LP1 1st class lab - CHAPTER TEST #3 PRACTICE LP1 #'d unknown tubes you do 10 smears on 1 tube and give me 3 perfect stains. 1 Gram, 1 AF, & 1 Endo 2nd class lab - LAST in class Practice for LP1 3 stains
Chapter Test #3 PRE-Lab Practical 1 Test 100 Multiple Choice + essay 2/3
Chapters 1-3+Scopes/Smears/Stains
Week 8
Week of 10/12 NO M40 the WEEKEND AFTER LP1
Chapter 9 Taxonomy
(video “Microbial Evolution) & Review for Lab Practical 1 Lecture material and Lab Staining Practice plus Demos of Metabolism Experiments
Lab Manual Cards DUE for Grading in Lab
Demos of Unknown Testing Procedure & Experiment Cards
READ "HOW TO START YOUR UNKNOWN TESTING!" online on the microblotsite: Pouring an Agar Plate, Streak Plate Isolation, "Dots-R-Us" lab, "Purity" Lab and Opt Temp Procedure Lab INOC/INCUB/EVAL
LAB MANUAL CARDS DUE in LAB for Grading: Lab Safety, Procedures and Experiments
LECTURE EXAM & LABORATORY PRACTICAL 1: full period testing; Intro Notes plus Chapters 1, 2, 3, + 9 and parts of 4 = 1 entire period MAJOR EXAM 1 - 200 multiple choice is Part A of this Exam; Unknown Bacteria smear stained with the 3 major stains and focused and explained thoroughly each slide evaluated in class is Part B of this exam; Problem Staining photographs is Part C of this exam (MC Part A only % also Counts as Chapter Test #4)
Week 9
Week of 10/19 M40 Friday 9 to noon over: Pouring an Agar Plate; Streak Isolation; "Dots-R-Us" Lab and Purity Lab.
Chapter 4 Cells continued
Chapter 5 Metabolism Lectures
Video “Metabolism”
Chapter 6 Growth Lectures
Unknown Isolation (Pouring an Agar Plate; Streak for Isolation; “Dots-R-Us & Purity Tests”)
Metabolism experiments –the Broths
1st class lab -Pouring an Agar Plate and Streak Isolation of Unknowns 2nd class lab - "Dots-R-Us" Lab, move to slants, incubation & Purity Testing + Opt Temp Lab (2 slants)
Pop Quiz INOC/INCUB/EVAL of Unknown Tests plus Chapters 5 and 6 notes
Week 10
Week of 10/26 M40 Friday 9 to noon Unknown Testing
Chapter 7 Genetics Lectures
Video “Reading DNA”
Discussion of Unknown Testing Broths, Slants, Deeps
1st class lab -"Purity Testing" and moving to 2 Opt Temp slants 2nd class lab -"Purity Testing of both Opt Temp slants and confirm Opt Temp; Begin inoc of BROTHS, SLANTS, and DEEPS
Chapter Test #5 PRE-LAB PRACTICAL evaluation = 100 multiple choice plus 2 short essays over Chapters 4, 5, 6 and ALL UNKNOWN PROCEDURE CARDS
Week 11
Week of 11/2 M40 Friday 9 to noon Unknown Testing, Library Assignment discussion, MT/LP2 Review
Chapter 8 Advanced DNA Lectures
Assigned video Worksheet: “The Mouse That Laid the Golden Egg”
Unknown Testing Broths, Slants, Deeps INOC/INCUB/EVAL 1st class lab & 2nd Lab = inoc and eval of broths, slants, and deeps
Pop Quiz Chapter 7/8 Unknowns
Week 12
Week of 11/9 NOVEMBER 11 Tues is a HOLIDAY- no classes
Lab Lecture Topic: How to determine the Genus & species of your Unknown 1st class lab & 2nd Lab = inoc and eval of broths, slants, and deeps
LIBRARY ASSIGNMENT DUE IN CLASS submitted BEFORE the MIDTERM/LP2 Exam
MIDTERM LECTURE EXAM AND LABORATORY PRACTICAL 2: full period testing; ALL Unknowns + Chapters 4, 5, 6, 7, 8 and parts of 9. 200 Multiple Choice, WORD Unknown Problems + 1 essay (MC% also counts as Chapter Test #6)
Week 13 Week of 11/16 LAST LAB M40 Friday 9-12meeting to END all Lab work, Confirm your Genus and species, & cleanup
Chapters 12 Sterilization, Ch 13 Antimicrobials, 14 – long lecture; short eval labs
Unknown Testing Plates and Disc Testing Ab/Antiseptics/Disinfectants INOC/INCUB/EVAL
Lab Lecture: “How to Write Your Formal Unknown Report”
1st class lab & 2nd Lab = inoc and eval of PLATE TESTS
LAB CLEAN-UP and Check-out Confirmation of GENUS and SPECIES from DATA
Pop Quiz Formal Unknown Report contents and format and Chapter 10/11
Week 14 Week of 11/23 M40 meetsFriday 9-11 "HOW TO TYPE YOUR UNKNOWN REPORT & FE review discussions"
Lecture Only – NO except clean-up and Confirmation of GENUS and SPECIES from DATA
Pop Quiz Chapters 12-15
Week 15 Week of 11/30 This is First Week in December after T-day NO more M40 11/27-28 Thanksgiving HOLIDAY WEEKEND - no classes THURS, FRI, SAT, SUN 11/27-29
Lectures on Chapters 17 and 18 Non-specific and Specific Immunity
Lecture only LACC clean-up and Confirmation of GENUS and SPECIES from DATA GCC Lecture 1 day and testing only the next class day – NO LAB
LACC PQ lecture Ch 15-16 GCCTyped Formal Unknown Report Due in class and Pre-graded during Chapter Testing 12/3
GCC Chapter Test #7 & 8: 200 multiple choice & 1 essay Chapters 10/11/12 Viruses + AIDS + Parasites and Sterilization
Week 16 Week of 12/7 GCC FINAL EXAM WEEK LACC Lectures, PAPER DUE & LAST CHAPTER TESTS plus wrap-up; Lab check-out LACC FINAL EXAM WEEK begins Monday Dec 15 the following week (see below) NO more M40
Lectures Chapters 15-18 LACC GCC FINAL EXAM DATE MONDAY DECEMBER 8 at 5:30-8 PM in SG-202 LACC lectures 1st class day; last Chapter Test#7 & 8 and Unknown Paper Due in class on the last class day 12/10-11
Lecture only LACC Labs ARE OVER! GCC Testing only Scantron 884E 200 multiple choice + FE Packet
GCC Final Exam Dec 8 at 5:30 PM - COMPREHENSIVE FINAL EXAM! 200 multiple choice questions – 150 most missed questions from Chapter tests and LP1/LP2MT plus 50 new questions from the new lecture material since The FE% also counts as Chapter Test 9
LACC Typed Formal Unknown ReportDue in class and Pre-graded during Chapter Testing 12/10-11
&
LACC Chapter Test #7 & 8: 200 multiple choice & 1 essay Chapters 10/11/12 Viruses + AIDS + Parasites and Sterilization
LACC Final Examyou choose the time and date (if not your regular class time then please email me for a seat #)
FE #1 Monday Dec 15 at 10-12:30 in SC-112
FE #2Tues Dec 16 at 1-3:30 PM in SC-112
FE#3Tues Dec 16 at 5:30-8 PM in SC-112
LACC Testing only Scantron 884E 200 multiple choice + FE Packet with your M40 take-home FE inside
LACC Final Exams Dec 15 & 16 ONLY - YOU CHOOSE in SG-112 - COMPREHENSIVE FINAL EXAM! 200 multiple choice questions – 150 most missed questions from Chapter tests and LP1/LP2MT plus 50 new questions from the new lecture material since The FE% also counts as Chapter Test 9
TheCOURSE CALENDAR(click on the yellow link to the left or see below) remember this must be RECONSTRUCTED each term and is quite lengthy - BE PATIENT - it takes a week or so!
Please note: (1) This calendar may change at any point (2) the Calendar is assumed to be accurate +/- 2 class periods (3) I will adjust the Calendar according to the speed of lecture and laboratory (4) If there is a particularly bad evaluation I may be repeat the TEST in the NEXT CLASS- be ready! and (5) THE DAILY WEBPAGE "WEEK IN BRIEF" ANNOUNCEMENTS followed by the DAILY AGENDA - "TRUMP" the CALENDAR if they conflict!
PAPERS SUBMITTED FOR GRADING
All papers submitted for grading must be typed. All submissions for grading must have the following information PRINTED in the upper right hand corner (or on side 1 of a Scantron in the NAME Box NOT ON THE BACK OF ANY SCANTRON!). Your PRINTED LAST name, printed first name; class name and section number (i.e., M-20#0930), the test/exam form letter and number (i.e., Exam 1A #34) if on a scantron and the date submitted. Besides Scantrons, all other submissions must be typed. On the first page place your name, class and section number and the date in the upper right corner of the first page. Pages must be numbered as well. Failure to follow these rules will result in -5 pts for EACH part of the rule omitted on each paper EVERY TIME you submit in error.
LECTURE & LABORATORY RULES & BEHAVIOR
Please be aware that some class lectures, labs and help sessions are videotaped for teaching purposes and improvement of instructions. By attending, students are consenting their permission to be filmed in a teaching situation.
Students may not enter any microbiology class or lab without the presence of the instructor or department staff. However, students may enter the classroom to wash hands, disinfect and seat themselvesifthe door is open. Student class Volunteers may enter to perform PRE-CLASS assignments as well - knock on the door of SC-110 & 112 if the rooms are locked and you arrive early to perform these tasks.
Students may not enter lecture or lab and work on lab assignments without permission. Lab work may continue during scheduled course times, only.
Food and/or drinks are not allowed in or during lab, whatsoever; and no visible cups, bottles, or food containers. Smoking, make-up application, texting, talking on cell phones, sleeping, or any other distracting behavior will also not be tolerated during lecture or lab. While microbes are present on the tables in the laboratory, all students must have their chairs "pushed" under the table-tops and be standing in proper lab attire (lab coats and gloves), if you need to exit the lab remove your lab attire - DO NOT WALK THE HALLS in lab attire. Note: the outside corridor doors are LOCKED during any active lab (if you are locked outside - knock on the door).
Lab spills should be disinfected immediately and the instructor notified. Glass breakage is NOT to be cleared by students - please spray disinfectant on the breakage and contact the instructor for assistance in cleaning.
VOLUNTEERS are sought for those taking the Microbiology-40 supplementary class who would like to perform before or end of class duties in liu of the LAB PREP HOUR requirement for their Microbiology 40 class. Students who wish to be an official "checker" or "recorder" must email such request to Professor Hicks and note this request on the class sign-in sheet during the first and second (1st & 2nd) week of class. If more than one request has been received, the position(s) will be assigned on a first-come basis from email requests
PLEASE treat everyone with respect and courtesy. Each and every student is expected to display equal and proper respect to others. Please avoid any overt or perceived actions that may be interpreted as prejudice or discrimination including but not limited to discrimination based on age, sex, religion, race, ethnicity, disability, sexual orientation or economic status. Such behavior will be grounds for immediate dismissal from class, pending administrative review.
CHEATING/TESTING: During all class evaluations, you will be seated randomly and your personal items are to be placed under or on the teacher tables at the front of the room - DO NOT LEAVE ITEMS IN THE WALKWAYS - place them on or under the tables. Instructions/Test Direction for each test will be found on each test. Failure to read these directions in their entirely may cause the loss of potential test points.To ensure students review this site daily, as required, tests will contain questions pertaining to the navigation of this site. Evaluations, including pop quizzes, will cover material discussed or assigned from the first to the last lecture day before the test. Please be aware that material in class will not follow the textbook and some lectures may incorporate material from a variety of chapters throughout the textbook, or from material found on handouts and videos.
Talking, whispering, cheat sheets, using electronic devices, changing graded answers, using false data, copying without referencing the source, copying another person's work, or exchanging different "forms" of a test during its administration is grounds for a zero (0) grade. If you received a (0), it is not because of an error. If you have a question about a grade, contact me by email or in class. If you have a question during an evaluation, raise your hand and then come and ask me quietly for the required information. Do not photograph exam question sheets without first obtaining permission. Do not ask for a bathroom break or any other "break" during evaluations - only in extreme emergencies will such request be allowed and those permitted shall leave their cell phone or other communication device in the classroom and be accompanied by a monitor.
Upon the belief of cheating, you will be asked to leave the class evaluation and evidence including witness statements will be collected. Subsequently, you will be contacted for a meeting to discuss the event with the instructor and the Dept. Head which could result in a charge of Academic Dishonesty by the college. Cheating on a required component of the course will result in the assignment of an (F) grade in the course. Since you are training to become health care workers,I take cheating very very seriously. PLEASE DO NOT CHEAT! If you have a problem, contact me prior to testing - contact me immediately - and I will do anything I can to help you succeed in the class!
ELECTRONIC DEVICES: All electronic devices must be turned off or set to vibrate prior to entering the classroom. However, students may voice-record lectures or use a laptop to take notes. Outside of Microbiology business, emailing, texting or chatting is not permitted on any device used during class lecture or laboratory.
10 Steps to an easy "A" in Microbiology:
(1) attend EVERY class including every Micro-40 Help, Lab Practice and Exam Review Session
(2) READ the assigned material in the textbook & in the notes the night BEFORE each lecture
(3) PRINT out the notes and bring them to class; fill-in any information not in the notes; ASK questions during lecture
(4) FORM a study group of 3-5 that meets weekly and reviews and discusses the notes and OLD TEST QUESTIONS. You can meet in M-40 in SC-112 on Fridays 9-12
(5) During testing READ every test question completely as there may be more than 1 correct answer (6) REVIEW any questions you miss on any test/evaluation and determine "why" you missed the question
(7) VOLUNTEER to be a class checker (this gets you an "A" in M-40 AND an "A" on the LRB)
(8) DO ALL the CLASS-WIDE BONUS POINT assignments on time and do them perfectly; do each evaluation BONUS POINT section
(9) REVIEW the most missed questions and any new material covered in class for the Comprehensive Final Exam
(10) Prepare your formal typed Unknown Report in advance by coming to the M-40 Unknown Report Review Session and turning it in on the last class day for PRE-GRADING (guaranteed 90%)
GRADES & GRADING
Students will receive one (1) warning about inappropriate use and setting(s) of their electronic devices. Further failure to observe course rules regarding electronic devices will cost the offending student ten (10) points per offense on that or the next evaluation.
Pop quizzes (PQs) could be given at any time. Pop quizzes are used to determine the final course grade in the case of BORDERLINE grade averages. Pop quizzes are 10-25 questions on a Scantron #882 and are composed 50% from what was covered in the last class and 50% over the assigned reading. Pop quiz answers will be provided upon request in the next class. Students may receive PQ points for submitting photos or short videos of any experiments - large numbers of good submissions that are used in class could equal a seventy-five percent (70%) PQ average and will meet the criteria for borderline "Push."Pop quiz Scantron grading is done during the last week of the term and the lowest 2 are dropped. If your pop quiz average is 70% or greater, then any decimal average will be increased to the next higher whole number i.e., 73.4% = 74% or 89.1% = 90%.
Students are expected to come prepared to any evaluation with a good #2 pencil with eraser and the required Scantron (#882 or #884) or supplies. Those who wish to change an answer may erase, remark and place a capital letter of their new answer over the letter (G) of their "Scantron".
Students will be dropped if two (2) complete class meetings are missed without an approved written excuse. Those who received an (I) in a previous term and are repeating or making up the course should not re-register but discuss which class they are going to attend with Professor Hicks. REMEMBER, After one (1) calendar year, a grade of (I) will default to the grade listed on the received academic notification, usually an (F) grade.
Your final average and final class grade is assigned by a computer - NOT BY ME. No one will receive any points outside those provided to each other student equally - DO NOT attempt to "mine" me for extra points. You will receive a MICROGRADESHEET to your official college email within 7-10 days after every evaluation - these become "official" within one week. Check your gradesheets and contact me immediately if suspect a discrepancy. After 1 week, these gradesheets become official college gradebooks and are not alterable.
Grades are assigned by the final weighted average in the class in the following manner: greater or = to 90% = A; 80-89% = B, 70-79% = C; 60-69% = D and equal or less than 59% = F. If you are likely to average a "C" in the class or below you will be advised to drop before the final drop day of your term.
The final weighted class average is made up of percent (%) scores from the following 4 class evaluation exercises:
(a) 3 major EXAMS valued at 20% of the total class grade (Lab Practical 1, MIDTERM/LabPractical 2, and a Comprehensive Final Exam - NOTE: no exam score is dropped),
(b) your biweekly Chapter Test average which counts as 25% of your total class grade (about 10 or more tests that are taken on a Scantron #882 and have about 50-100 questions + 2 essay tests; the lowest 2 Chapter test scores are dropped; each EXAM score is also recorded as a Chapter Test score but may be dropped as a lowest score in this category only),
(c) a Laboratory Record Book (LRB) which counts 2%, and
(d) an APA-style typed formal Unknown Report which counts 13%.
There are CLASS-WIDE BONUS points to be earned in this class which add 2-3% (depending on the term and the Dept Head rules) on top of your weighted average. They are: (1) your homemade Lab Unknown Test Manual (50 pts), (2) the Unknown Library Assignment (25 pts) and (3) the Parasite Assignment (25 pts).
Each test/exam or evaluation may also have an individual BONUS question or 2 which applies to that test or exam ONLY and not to your weighted class average.
*Please note that each major Exam percent score ALSO is recorded as a Chapter Test Score and the MT is recorded 3 times...once as a total MT exam score (MC+Bonus Word problems = your MT Exam score which is 20% of your final grade) and once as LP2 from the multiple choice portion of the test as well as once with the multiple choice as a chapter test for the chapter material. Any recorded Chapter Test Score can be dropped and the lowest 2 are dropped automatically by the computer program. The LRB score and Unknown Paper are not recorded as a Chapter Test Score.
LECTURE & LAB SEATING/Daily Procedures
Official class seating will be assigned at the conclusion of the second (2nd) week of the term. All seating for lectures and lab is by alphabetical order according to last name. Each class day, students are to leave their belongings in their assigned chairs, wash their hands (well) at the sink and wipe down the tabletop with the provided disinfectant before touching the tabletops. Please use the same paper used to dry hands to smear the disinfectant around the tabletop and let it air-dry. Prior to exiting lab, students are to complete these actions in reverse. Please do not leave the lab wearing smocks and/or gloves on, as it "frightens the natives in the halls." When microbes are present, students must be in lab attire (lab coats + gloves) and the chair are to be "pushed" under the table tops (put your things in the chairs), the room doors are locked and the tabletops are disinfected with only the LRB and or lab materials left available on top for student use.
FINAL EXAMINATIONS
Students enrolled in Microbiology 40 must complete the course' final exam and include it in their final exam packet on the scheduled final exam day.
Students in M-20 and M-1 may select their final lecture exam date and time from the dates my finals are offered which will be listed here on this site during the week before Final exams. Course Final Exams are comprehensive 200 multiple choice question exams using a Scantron #884E only. There are no Bonus or Essay/short answer questions on the Final Exam. The questions are derived from any new material covered since the last evaluation plus questions selected from those used in previous evaluations.
NO MORE THAN 4 mis-erasers 2X during any term will be applied to your grade. Learn to mark carefully. When I see cheating I take witness statements as well as the "Proctor's" statement... Then, I apply the consequences. If you wish to challenge this please make an appointment by email!
Beginning in Week 3 the VOLUNTEER Checkers should do the scopes before and after class and the Room/Sink Checkers should check the room, clean the sinks, and re-fill the stains, lens paper containers, and disinfectant bottles each day! IF YOU ARE A "CHECKER" have me SIGN your LRB during the LAST week of the term - AFTER you have done your assignment!
Please don't email questions that can be found by viewing this INDEX PAGE! Or if you have not copied the board agenda daily - LOOK IN YOUR LRB or here. If the dates/info is in CONFLICT - the MASS EMAIL wins all followed by the INDEX PAGE. Why? Because individual classes may move faster or slower than our planned daily agenda acccounts for...
I may not have time to answer every Google+ posts however...I WILL TRY! Remember, I have no time to answer hundreds of questions on the day of exams. The tests are given in day pairs... Monday/Tuesday or Wed/Thurs. ----- so if you want information ask on Google+ bySundayfor the next week's test...
ALL SCANTRON TESTS are graded ASAP and Grade sheets are returne/updated about every 7-10 days... check your email. If you find an error on your SCANTRON or GRADESHEET, circle the scantron number in RED pen and return it to me ASAP. If the error is on your gradesheet, print out the gradesheet and circle the error in RED and bring it to me in your next class... NOTE: All scantrons/essays/evaluation materils are SCANNED by me before I return them to you for review and consideration for the Final Exam. DO NOT ALTER ANY SUBMITTED MATERIAL as they are checked for alterations. Any "bogus" changes/faked errors will result in a dishonesty measure (grade recorded as a "0")
HOW TO BEGIN ORGANIZING FOR A NEW TERM!
Over the years, I have added a number of things to the class besides the usual textbook, lecture, and lab exercises. The first was to delete the cost and waste of a lab manual (you make your own using the Microwebsite/microblogsite) and the design of a class website. The Microblogsite assists you in obtaining copies of many class materials that you might not normally be able to access. I have added many other features and ancillary materials since and more are to come.
Remember the assistance provided below is NOT REQUIRED of me, I do it because I want YOU to do well in the class and to make it easier and more adaptable to the changing requirements of Science. HOWEVER, I am not a computer designer/engineer and my learning curve is steep. Things may not work perfectly for everyone or anyone and alterations may be needed instantly to make our ideas/technology work or continue to work. Try, ask, be flexible and it will help us all!
IMPORTANT:The MICRODROPBOX link below contains a number of important ancillary materials including: video lectures, audio lectures, copies of old test questions, helpful study charts, old editions of texts, as well as the class POWERPOINTS.
Here are the resources I have designed and/or provide:
(1) Class notes from the outlines/Pdf's/PowerPoints used in lecture
(2) Instructions on how to do the labs and what they teach as well as what things "look like"
(3) An interactive chat/display site for 24/7 communication, questions & visualizations of the classwork- GOOGLE+
(4) Copies of MY old test questions that you can use - NOT FOR MEMORIZATION, but to check your progress and to learn HOW I ask questions on exams -
(5) Videos of the lecture material and labs - MICROBLOGSITE UTUBE LIST
(6) NEW material -- as SCIENCE changes by the minute
(7) NEW teaching/electronic media presentations as this is also changing almost daily!
(8) Example Term Papers and assistance with writing the required class term paper - MICROBLOGSITE BUTTON
(9) Forums/discussion sites for interaction and solutions of hardware/software problems - Microwebsite/GOOGLE+
(10) A monthly email of your current GRADES on a privately emailed gradesheet...
(11) Instant email notice of changes/concerns/announcements - MASS CLASS EMAIL/Google+
(12) A student email address dedicated ONLY to students which is monitored constantly!
I have a lot of work to do! I am trying to make this site open and useful for you and me. Google has created a limited access owner controlled Google+ Community which will allow me to control the content and members more closely. I am trying to teach myself how to create it and move the materials from the current one.
RE-GAINING minus points taken on any 1 test or exam - GRADING ON "FAILURE TO FOLLOW TEST DIRECTIONS": You can return one (1) paper that I have taken off points for recording infractions once by putting it in your Final Exam packet and I will give them back ONCE on 1 paper only! I will NOT return points for cheating or writing on exams. I WILL NOT MAKE CORRECTIONS ON SCANTRON ERASERS MORE THAN up to 4 erasers on 1 paper per term! If you do not buy a better eraser and learn to erase and remark.. you will have to retake the exam using a different version of the exam. No more than 4 erasers on 1 test ONCE. If there is another dispute you may request to retake another version of the Exam after the second instance of "misgrades"
* During your first class your instructor will give you the ID and Password to enter the MicroWebsite; EMAIL me if you have forgotten...
Email Address for Students ONLY (PLEASE USE!): hicksmicro@gmail.com ---- DO NOT USE MY LACITYCOLLEGE.EDU address
The LACC MICROBIOLOGY LECTURE/ LAB Room is located in the SC Building in Room #112.
The LACC MICROBIOLOGY PREP ROOM is located in the SC Building in Rm #110.
This room is used for the Lab Tech Lab Assistant and is where you will have at least 10 hours of laboratory preparation training (usually 9-12 only on FRIDAY). EMERGENCY TEXT number: 213-377-4456
Sheriff's Office EMERGENCY TELEPHONE NUMBER: 323-662-5276 or from a campus phone press #3; call the LA CITY COLLEGE Sheriff's Office BEFORE 911!
BOSTON -- A long-acting injectable drug could be the Depo-Provera of anti-HIV drugs.
The data on GSK744 -- albeit still mostly from animal studies -- are "really exciting" and hold the promise of improving the real-world performance of pre-exposure prophylaxis, or PrEP, commented Sharon Hillier, PhD, of the University of Pittsburgh, who moderated a press conference at the Conference on Retroviruses and Opportunistic Infections.
With more study, Hillier said GSK744 could be "almost like a Depo-Provera-type shot" -- given every few months to prevent HIV infection, just as Depo-Provera is given to prevent pregnancy.
But "taking a pill once a day can be challenging for some people," said Gerardo Garcia-Lerma, PhD, of the CDC in Atlanta, senior author of one of the papers presented here.
The hypothesis is that long-acting drugs might "improve adherence and thus PrEP efficacy," said Chasity Andrews, PhD, of the Aaron Diamond AIDS Research Center in New York City, lead author of the Science paper and two of the presentations here.
In principle, such long-acting drugs could also be used for treatment of HIV infection, although that would require more than a single medication. But at the moment, there is another obstacle -- the drug is given in two intramuscular injections, one in each gluteal muscle, Hiller explained.
"I think it's probably a little way before people start lining up to get a 2 milliliter injection in each gluteal at really frequent intervals, outside of the high-risk setting," she said.
Formulations are likely to improve, but the main interest in the long-acting drugs is still to prevent infection in the first place, especially in people at high risk, commented Sharon Lewin, MD, of Monash University in Melbourne, Australia, who is co-chair of the International AIDS conference this year in Melbourne.
The issue is adherence as most people at high risk for HIV are still healthy and their motivation to take a daily pill varies from time to time, Lewin told MedPage Today.
"Your motivations are very different when you're infected," she said. "But asking a young healthy guy to take a pill every day is really tricky."
To make sure PrEP works, "you need a delivery system that is less operator-dependent," she said, and drugs like GSK744 might do the trick.
GSK744 is an integrase strand-transfer inhibitor, an analog of the recently approved dolutegravir (Tivicay). It can be formulated as a nano-suspension that had a half-life of 21 to 50 days in healthy human volunteers.
Both Andrews and Garcia-Lerma reported on the effect of the drug in preventing macaques from acquiring SHIV -- a constructed amalgam of HIV and the simian immunodeficiency virus, or SIV.
The experiments demonstrated a consistent protective effect whether the challenge was rectal or vaginal, they said.
PrEP studies in humans are in the planning stage, Andrews said.
The study by Andrew's group was partly funded by NIH and the Tulane National Primate Research Center.
Some co-authors are employees of GlaxoSmithKline (GSK) and hold company shares. One co-author reported being a paid consultant to GSK.
One co-author reported serving on the ViiV Healthcare Bo
HOW IS TRUVADA USED
TO TREAT HIV-1 INFECTION?
TRUVADA is a type of medicine called a nucleoside analog reverse transcriptase inhibitor (NRTI) that is used to treat HIV-1 infection in adults and teenagers (12 and older).
TRUVADA is a combination therapy because it has 2 medicines in 1 pill– emtricitabine and tenofovir disoproxil fumarate. TRUVADA is always used with other anti-HIV medicines to treat HIV-1 infection because TRUVADA alone is not a complete treatment.
Understanding HIV
HIV infects important cells for fighting infection called CD4 cells, or T cells. Once HIV enters the body, the virus multiplies inside these cells. These new viruses are released into the blood and infect other CD4 cells.
How TRUVADA can help
When used with another anti-HIV-1 medicine, TRUVADA helps make it harder for HIV-1 to multiply by blocking an enzyme in your body called reverse transcriptase
By helping to keep HIV-1 from multiplying in your body, TRUVADA helps lower the viral load, which means decreasing the amount of HIV in the blood
TRUVADA may also help increase the number of CD4 cells when used with another anti-HIV-1 medicine
TRUVADA is a prescription medicine used in 2 different ways:
to treat HIV-1 infection in adults and teenagers (12 and older). When used for the treatment of HIV-1 infection, TRUVADA is always used together with other HIV-1 medicines.
to help reduce the risk of getting HIV-1 infection when used together with safer sex practices. This use is only for adults who are at a high risk of getting HIV-1. This includes HIV-negative men who have sex with men and who are at high risk of getting infected with HIV-1 through sex, and male-female sex partners when one partner has HIV-1 and the other does not.
TRUVADA does not cure HIV-1 infection or AIDS. Ask your healthcare provider if you have questions about how to prevent getting HIV-1 or passing HIV-1 to others. Always practice safer sex and use condoms to lower the chance of sexual contact with body fluids. Never reuse or share needles or other items that have body fluids on them. If you are taking TRUVADA with other HIV-1 medicines to treat HIV-1, you must keep taking TRUVADA to control HIV-1 infection and decrease HIV-1 related illnesses.
IMPORTANT SAFETY INFORMATION
What is the most important information I should know about TRUVADA?
TRUVADA can cause serious side effects:
Too much lactic acid in your blood (lactic acidosis), which is a serious medical emergency. Symptoms of lactic acidosis include weakness or being more tired than usual, unusual muscle pain, being short of breath or fast breathing, nausea, vomiting, stomach-area pain, cold or blue hands and feet, feeling dizzy or lightheaded, and/or fast or abnormal heartbeats.
Serious liver problems. Your liver may become large and tender, and you may develop fat in your liver. Symptoms of liver problems include your skin or the white part of your eyes turns yellow, dark “tea-colored” urine, light-colored stools, loss of appetite for several days or longer, nausea, and/or stomach-area pain.
You may be more likely to get lactic acidosis or serious liver problems if you are female, very overweight (obese), or have been taking TRUVADA for a long time. In some cases, these serious conditions have led to death. Call your healthcare provider right away if you have any symptoms of these conditions.
Worsening of hepatitis B (HBV) infection. If you also have HBV and take TRUVADA, your hepatitis may become worse if you stop taking TRUVADA. Do not stop taking TRUVADA without first talking to your healthcare provider. If your healthcare provider tells you to stop taking TRUVADA, they will need to watch you closely for several months to monitor your health. TRUVADA is not approved for the treatment of HBV.
If your healthcare provider has prescribed TRUVADA to help reduce the risk of getting HIV-1 infection, you should also know:
You must be HIV-negative before you start taking TRUVADA to reduce the risk of getting HIV-1. You must get tested to make sure that you do not already have HIV-1 infection. Do not take TRUVADA to reduce the risk of getting HIV-1 unless you are confirmed to be HIV-negative.
Many HIV-1 tests can miss HIV-1 infection in a person who has recently become infected. If you have flu-like symptoms, you could have recently become infected with HIV-1. Tell your healthcare provider if you had a flu-like illness within the last month before starting TRUVADA or at any time while taking TRUVADA. Symptoms of new HIV-1 infection include tiredness, fever, joint or muscle aches, headache, sore throat, vomiting, diarrhea, rash, night sweats, and/or enlarged lymph nodes in the neck or groin.
Just taking TRUVADA may not keep you from getting HIV-1. You must continue using safer sex practices while you are taking TRUVADA to reduce your risk of getting HIV-1. To further reduce your risk of getting HIV-1:
Get tested for other sexually transmitted infections. Other infections make it easier for HIV-1 to infect you.
Get information and support to help reduce risky sexual behavior.
Have fewer sex partners.
Do not miss any doses of TRUVADA. Missing doses may increase your risk of getting HIV-1 infection.
You must stay HIV-negative to keep taking TRUVADA to reduce your risk of getting HIV-1:
Know your HIV-1 status and the HIV-1 status of your partners.
Get tested for HIV-1 at least every 3 months or when your healthcare provider tells you.
If you think you were exposed to HIV-1, tell your healthcare provider right away.
If you do become HIV-1 positive, you need more medicine than TRUVADA alone to treat HIV-1. TRUVADA itself is not a complete treatment for HIV-1.
If you have HIV-1 and take only TRUVADA, your HIV-1 may become harder to treat.
If your healthcare provider has prescribed TRUVADA to help reduce the risk of getting HIV-1 infection, do not take TRUVADA if:
You already have HIV-1 infection or if you do not know your HIV-1 infection status. If you are HIV-1 positive, you need to take other medicines with TRUVADA to treat HIV-1. TRUVADA itself is not a complete treatment for HIV-1. If you have HIV-1 and take only TRUVADA, your HIV-1 may become harder to treat.
What are the other possible side effects of TRUVADA?
Serious side effects of TRUVADA may also include:
New or worsening kidney problems, including kidney failure. Your healthcare provider may do blood tests to check your kidneys before and during treatment with TRUVADA. If you develop kidney problems, your healthcare provider may tell you to take TRUVADA less often, or to stop taking TRUVADA.
Bone problems, including bone pain or bones getting soft or thin, which may lead to fractures. Your healthcare provider may do tests to check your bones.
Changes in body fat can happen in people taking HIV-1 medicines.
Changes in your immune system. If you have HIV-1 infection and start taking HIV-1 medicines, your immune system may get stronger and begin to fight infections. This may cause minor symptoms such as fever, but can also lead to serious problems. Tell your healthcare provider if you have any new symptoms after you start taking TRUVADA.
The most common side effects of TRUVADA are:
In people taking TRUVADA with other HIV-1 medicines to treat HIV-1 infection, common side effects include: diarrhea, nausea, tiredness, headache, dizziness, depression, problems sleeping, abnormal dreams, and rash.
In people taking TRUVADA to reduce the risk of getting HIV-1 infection, common side effects include: headache, stomach-area (abdomen) pain, and decreased weight.
Tell your healthcare provider if you have any side effects that bother you or don’t go away.
What should I tell my healthcare provider before taking TRUVADA?
All your health problems. Be sure to tell your healthcare provider if you have or had any kidney, bone, or liver problems, including hepatitis virus infection.
If you are pregnant or plan to become pregnant. It is not known if TRUVADA can harm your unborn baby. Tell your healthcare provider if you become pregnant while taking TRUVADA. If you are taking TRUVADA to reduce the risk of getting HIV-1 and you become pregnant, talk to your healthcare provider to decide if you should keep taking TRUVADA.
If you are breastfeeding (nursing) or plan to breastfeed. Do not breastfeed. HIV-1 can be passed to the baby in breast milk. Also, the medicines in TRUVADA can pass into breast milk, and it is not known if the medicines can harm the baby.
All the medicines you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements. TRUVADA may interact with other medicines. Keep a list of all your medicines and show it to your healthcare provider and pharmacist when you get a new medicine.
Your healthcare provider may need to check you more often or change your dose if you take any of these medicines with TRUVADA: didanosine (Videx EC), atazanavir (Reyataz), darunavir (Prezista), or lopinavir with ritonavir (Kaletra).
You are encouraged to report negative side effects of prescription drugs to the FDA. Visit www.FDA.gov/medwatch, or call 1-800-FDA-1088.
Guidelines have been updated to reflect the fact that people with HIV are now living normal life spans. In addition to routine HIV management, the guidelines emphasize that clinicians focus on preventive care for other serious health conditions.
According to the CDC, nearly 1.2 million Ameri-cans are living with HIV and about 50,000 people in the United States are infected with the virus each year. Studies have estimated that as many as 80% of patients with HIV have their virus under control and live long, full lives. “With HIV continuing to become a manageable but complex chronic disease, HIV specialists and primary care physicians (PCPs) now need to provide the full spectrum of healthcare to these patients,” says Michael A. Horberg, MD, MAS, FACP, FIDSA. “PCPs and other healthcare providers need a better grasp of the impact that HIV care has on routine healthcare.”
A Helpful Update
In 2009, an expert panel of the HIV Medicine Association of the Infectious Diseases Society of America (IDSA) released evidence-based guidelines for the management of people infected with HIV. Recently, these guidelines were updated to replace the 2009 recommendations and published in Clinical Infectious Diseases. Since 2009, new antiretroviral drugs and classes have become available, and the prognosis of people with HIV infection continues to improve. The guideline update also incorporates new information based on publications from 2009 to 2013.
“The updated IDSA guidelines are intended for use by healthcare providers who care for HIV-infected patients,” says Dr. Horberg, who was on the expert panel that developed the update. “These new recommendations reflect the fact that people with HIV are now living much more normal life spans. As such, there is a greater need to focus on preventive care, including screening for high cholesterol, diabetes, osteoporosis, depression, and substance abuse, among other health conditions.”
Although there are better survival rates, people with HIV are increasingly developing common health problems that also affect the general population. Some of these conditions may be related to HIV infection itself or its treatment. “An important theme of the guidelines is that HIV-infected patients be managed and monitored for all relevant age- and sex-specific health problems,” Dr. Horberg says.
Summarizing Key Changes
The guidelines have expanded recommendations on the initial evaluation and immediate follow-up for HIV-infected patients. Patients whose infection is under control for some time can have their HIV blood levels monitored every 6 to 12 months, rather than every 3 to 4 months as previously recommended (Table 1). In addition, the guidelines include new recommendations on screening for diabetes, osteoporosis, and colon cancer. They also suggest that patients with HIV infection be vaccinated against pneumococcal infection, influenza, varicella, and hepatitis A and B. “HIV may be under control in many patients, but we still should stress the importance of preventing other health problems,” adds Dr. Horberg. “This requires taking a holistic approach to care.”
The IDSA’s guideline update has added easy-to-use tables that outline interactions between specific antiretroviral drugs and statins. Importantly, a new section on metabolic comorbidities was added to the guidelines, replacing the need for separate recommendations on dyslipidemia, which had been previously published (Table 2). There also is a more robust section on sexually transmitted diseases, including a recommendation for annual screening of trichomoniasis in women and yearly screening for gonorrhea and chlamydia for patients considered to be at risk.
Behavior Matters
“The guidelines stress that physicians should consistently discuss and counsel patients on their sexual history and any risky behaviors, such as using illicit drugs,” Dr. Horberg says. “We need to do this in a non-judgmental manner. We also need to determine how well patients are coping with living with HIV and if they have a sufficient support network.” General messages about risk reduction should be provided at all healthcare encounters—regardless of risk behaviors—by providers, others in healthcare, or with educational materials (eg, pamphlets, posters, and videos). Tailored messages are critical, especially for patients persistently reporting high-risk behaviors. Referrals to programs capable of offering more extensive interventions are also important.
When HIV is under control, patients often feel that they do not need to see their physicians regularly. Dr. Horberg says adherence is about more than just taking HIV medications on a regular basis. “It’s also about receiving regular primary care,” he says. “HIV specialists and PCPs alike need to be familiar with these issues so that we can bridge treatment gaps in HIV care. These guidelines are designed to help ensure that patients with HIV live long and healthy lives. Hopefully, we can learn more about methods for further enhancing our ability to take a holistic approach to caring for patients infected with HIV.”
Additional Resources:
Aberg JA, Gallant JE, Ghanem KG, Emmanuel P, Zingman BS, Horberg MA. Primary care guidelines for the management of persons infected with HIV: 2013 update by the HIV Medicine Association of the Infectious Diseases Society of America. Clin Infect Dis. 2013 Nov 14 [Epub ahead of print].
AIDSinfo. Guidelines for prevention and treatment of opportunistic infections in HIV-infected adults and adolescents, 2013. Available at: http://aidsinfo.nih.gov/guidelines/.
Dube MP, Stein JH, Aberg JA, et al. Guidelines for the evaluation and management of dyslipidemia in human immunodeficiency virus (HIV)–infected adults receiving antiretroviral therapy: recommendations of the HIV Medical Association of the Infectious Diseases Society of America and the Adult AIDS Clinical Trials Group. Clin Infect Dis. 2003;37:613-627.
Aberg JA, Kaplan JE, Libman H, et al. Primary care guidelines for the management of persons infected with human immunodeficiency virus: 2009 update by the HIV Medicine Association of the Infectious Diseases Society of America. Clin Infect Dis. 2009;49:651-681.
- See more at: http://www.physiciansweekly.com/hiv-guidelines-2013/?utm_source=Physician%27s+Weekly+eNewsletter&utm_campaign=f7afe2e8ab-ID_Hospitalists_CC_Cubicin-3_25_14&utm_medium=email&utm_term=0_35606603ab-f7afe2e8ab-108543397#sthash.Iovy7ctr.dpuf
Chitosan microparticles—derived from dissolved shrimp shells—kill bacteria in cows’ uteri and may someday be used to help people who have become ill from consuming E. coli-contaminated food. (Credit: Dave Wild/Flickr)
Mooo! SHRIMP SHELLS MAY SHIELD COWS (AND PEOPLE) FROM
E. coli.
A new biological treatment could help dairy cattle stave off uterine diseases and eventually may help improve food safety for people, new research suggests.
Cattle uterine illnesses can make cows infertile and lower milk production, maladies that are often linked to bacteria.
For a new study, researchers infused chitosan microparticles—an antimicrobial material derived from dissolved shrimp shells—into diseased cow uteri. When bought in stores, chitosan can be used to treat a variety of ailments, including obesity and anemia.
On its own, chitosan only works at acidic pH levels. For cattle, the researchers developed chitosan microparticles, which work in acidic and neutral pH, because cattle uteri have a neutral pH.
Published in PLoS One, the findings suggest chitosan microparticles kill bacteria in the uteri. It may someday be possible for chitosan microparticles to be used to help humans who have become ill from consuming E. coli-contaminated food, but more research is needed.
Developing a new antimicrobial agent is critical to human and animal health, says Kwang Cheol Jeong, an assistant professor in animal sciences at the University of Florida.
“Dangerous infections are diminishing the role of some antibiotics, making them less able to treat infections, as pathogens are developing resistance to the drugs,” he says, adding that about 23,000 people die in the US annually because of exposure to pathogens that don’t respond to antibiotics.
GOOD AND BAD BACTERIA
Once bacteria become resistant, whether on farms, hospitals, or in the environment, they can infect humans, through water, food, or contact with contaminated feces.
Further, some antibiotics used to treat humans and animals kill good and bad bacteria. Scientists can use the new study’s findings to begin to develop better drugs that target bad pathogens but leave beneficial bacteria.
E. coli are everywhere, including the human gut, but can contaminate beef, unpasteurized milk, soft cheeses made from raw milk, and raw fruits and vegetables that haven’t been washed properly.
The most recent outbreak of meat-traced E. coli was in 2010, according to the Centers for Disease Control and Prevention. That year, 21 people in 16 states fell ill from the pathogen. A foodborne “outbreak” happens when two or more people get the same Reaseachers Report Treatment Clears HIV in Second Baby
Published: Mar 5, 2014 | Updated: Mar 6, 2014
By Michael Smith, North American Correspondent, MedPage Today
BOSTON -- Evidence is increasing that treating HIV-positive babies within a few hours of birth can dramatically restrict -- and perhaps eliminate -- infection, a researcher said here.
After nearly 2 years off anti-HIV therapy, the so-called Mississippi baby -- now 41 months old -- remains free of HIV, according to Deborah Persaud, MD, of Johns Hopkins University.
The first reports of the case were met with "skepticism and optimism," Persaud told reporters, but they prompted physicians in Los Angeles County to initiate very early treatment for a child born there to an HIV-positive mother.
The baby, born at Long Beach's Miller Children's Hospital, was given triple drug HIV therapy starting within 4 hours of birth to a mother with untreated HIV.
Tests at birth showed the presence of HIV DNA in the baby and testing 36 hours later -- 32 hours after treatment was started -- showed a plasma viral load of 217 copies per milliliter. A spinal tap when the child was 6 days old showed 32 copies of HIV RNA per milliliter of cerebrospinal fluid, Persaud reported.
But within days, almost all signs of HIV had disappeared. The plasma viral load, for instance, was and has remained undetectable, defined as fewer than 20 copies per milliliter.
Importantly, Persaud said, there is no indication that the child harbors a reservoir of "replication-competent virus" even if fragments of HIV RNA or DNA are present.
The child -- unlike the Mississippi baby -- has been kept on therapy, so investigators can draw no conclusions about whether the virus has been beaten permanently, Persaud said.
She told MedPage Today that there are no immediate plans to interrupt treatment for the Long Beach child, although her care team has initiated "conversations" about the issue with their institutional review board.
If there is "some consensus" that the anti-HIV medications should be stopped, it would happen when the child reaches age 2, she said. In the Mississippi case, the stoppage was inadvertent, after the child was lost to follow-up.
The two cases are a "signal that giving very early treatment to neonates really restricts HIV spread to the point where it is difficult to detect infection," she said.
Persaud added that plans are underway for a prospective international clinical trial involving 54 infants who will be treated at birth or very soon after, with planned treatment interruptions at age 2.
The report is an additional signal that very early treatment might interrupt the "seeding" of the HIV reservoir, commented Elaine Abrams, MD, of Columbia University in New York City, who was not part of the study but who moderated a press conference at which some details were reported.
"How limiting the reservoir will relate to remission and cure is still to be tested," she toldMedPage Today. "What happens when this kid stops drugs -- and I suspect they eventually will -- will be interesting to see."
Abrams noted that other studies have shown that starting therapy at 6 to 12 weeks of age is too late. "When you stop therapy at 2 years later, you get virus," she said.
Scientists have successfully genetically engineered the immune cells of 12 HIV positive patients to resist infection, and decreased the viral loads of some patients taken off antiretroviral drug therapy (ADT) entirely—including one patient whose levels became undetectable.
The study, which appears today in the New England Journal of Medicine, is the first published report of any gene editing approach in humans.
“This study shows that we can safely and effectively engineer an HIV patient’s own T cells to mimic a naturally occurring resistance to the virus, infuse those engineered cells, have them persist in the body, and potentially keep viral loads at bay without the use of drugs,” says senior author Carl H. June, professor in immunotherapy at the University of Pennsylvania Perelman School of Medicine.
“This reinforces our belief that modified T cells are the key that could eliminate the need for lifelong ADT and potentially lead to functionally curative approaches for HIV/AIDS.”






 Truvadais a type of medicine called a nucleoside analog reverse transcriptase inhibitor (NRTI) that is used to treat HIV-1 infection in adults and teenagers (12 and older).
Truvadais a type of medicine called a nucleoside analog reverse transcriptase inhibitor (NRTI) that is used to treat HIV-1 infection in adults and teenagers (12 and older).